

Significance of nutritional status in the development of periprosthetic infections : A retrospective analysis of 194 patients
- PMID: 32424439
- PMCID: PMC7925508
- DOI: 10.1007/s00132-020-03922-8
Significance of nutritional status in the development of periprosthetic infections : A retrospective analysis of 194 patients
Abstract
Background: Malnutrition caused by protein and vitamin deficiencies is a significant negative prognostic factor in surgical wound healing disorders and infections. Particularly in elective surgery, preoperative compensation of deficiencies is advisable to avoid negative postoperative consequences. This study examined the nutritional and protein balance of patients with periprosthetic hip and knee joint infections.
Material and methods: Patients with periprosthetic hip or knee joint infections constituted the study group (SG). Control group I (CG I) included patients with primary implants and CG II included patients who required revision surgery because of aseptic loosening. Relevant nutritional and protein parameters were determined via analysis of peripheral venous blood samples. In addition, a questionnaire was used to evaluate the nutritional and eating patterns of all patients. The nutritional risk screening (NRS) 2002 score and body mass index (BMI) were also calculated for all participants.
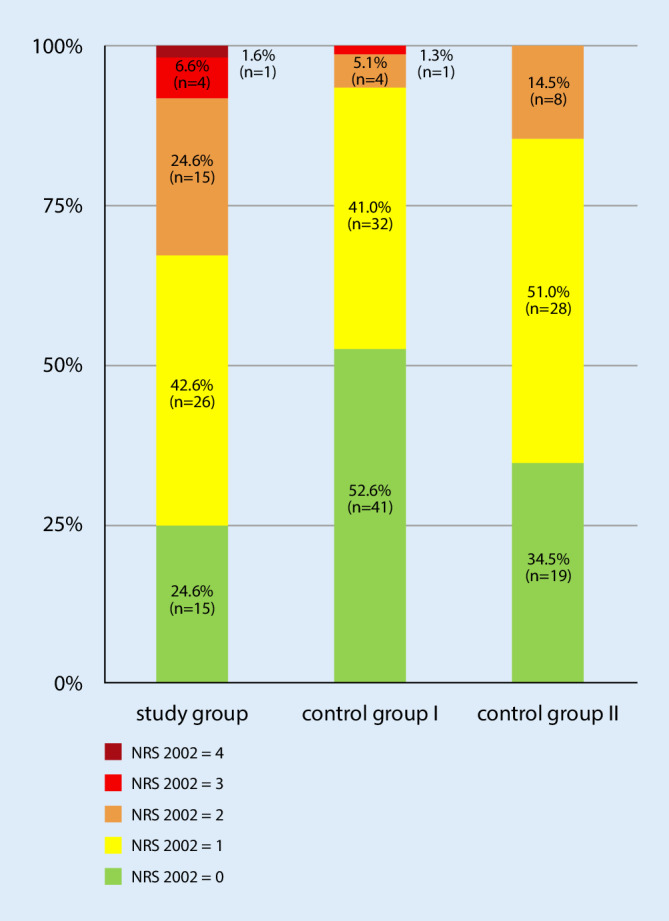
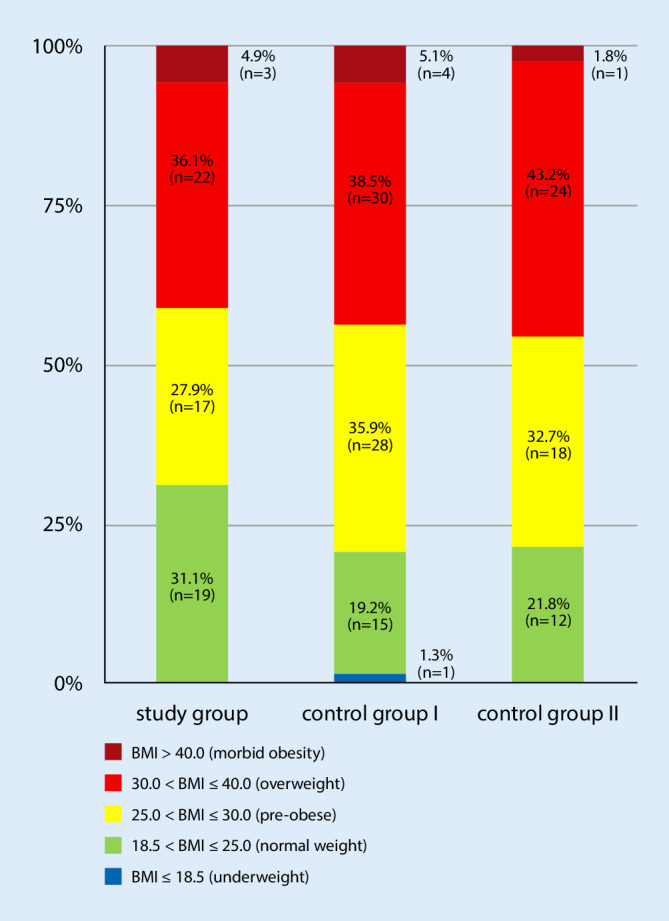
Results: Differences were found in the albumin level (SG: 36.23 ± 7.34, CG I: 44.37 ± 3.32, p < 0.001, CG II: 44.06 ± 4.24, p < 0.001) and total protein in serum (SG: 65.42 ± 8.66, CG I: 70.80 ± 5.33, p = 0.004, CG II: 71.22 ± 5.21, p = 0.004). The number of patients with lowered albumin levels (SG 19/61, CG I 1/78, CG II 2/55) and total protein in serum (SG: 12/61, CG I 5/78, CG II 2/55) also showed considerable variation. The number of patients with a NRS 2002 score ≥3 differed significantly between SG and both CGs (SG: 5/61, CG I 1/78, CG II 0/55); however, these differences could not be confirmed using BMI.
Conclusion: As expected, lowered albumin and total protein levels were observed in PJI due to the acute phase reaction. The NRS can be performed to exclude nutritional deficiency, which cannot be excluded based on BMI. In cases of periprosthetic joint infection it is reasonable to compensate the nutritional deficiency with dietary supplements.
Zusammenfassung: HINTERGRUND: Unterernährung aufgrund von Protein- und Vitaminmangel ist ein bedeutender negativer Prognosefaktor bei chirurgischen Wundheilungsstörungen und Infektionen. Insbesondere bei elektiven Eingriffen ist ein präoperativer Ausgleich von Mangelerscheinungen ratsam, um negative postoperative Folgen zu vermeiden. Ziel dieser Studie war es, die Ernährungs- und Proteinbilanz von Patienten mit periprothetischen Hüft- und Kniegelenkinfektionen zu untersuchen.
Material und methoden: Patienten mit periprothetischen Hüft- oder Kniegelenksinfektionen bildeten die Studiengruppe (SG). Die Kontrollgruppe I (CG I) umfasste Patienten mit Primärimplantaten, während die CGII Patienten einschloss, die wegen aseptischer Lockerung eine Revisionsoperation benötigten. Bei allen Patienten wurden relevante Ernährungs- und Proteinparameter durch die Analyse von Blutproben bestimmt. Darüber hinaus wurde ein Fragebogen zur Bewertung der Ernährungs- und Essgewohnheiten aller Patienten erhoben. Der Score des Nutritional Risk Screening (NRS) 2002 und der Body-Mass-Index (BMI) wurden ebenfalls für alle Teilnehmer bestimmt.
Ergebnisse: Unterschiede wurden im Albuminspiegel (SG: 36,23 ± 7,34, CG I: 44,37 ± 3,32; p < 0,001; CG II: 44,06 ± 4,24, p < 0,001) und im Gesamtprotein im Serum festgestellt (SG: 65,42 ± 8,66, CG I: 70,80 ± 5,33; p = 0,004; CG II: 71,22 ± 5,21; p = 0,004). Die Anzahl der Patienten mit erniedrigten Albuminwerten (SG: 19/61, CG I: 1/78, CG II: 2/55) und des Gesamtproteins im Serum (SG: 12/61, CG I: 5/78, CG II: 2/55) zeigten ebenfalls beträchtliche Unterschiede. Die Anzahl der Patienten mit kritischem Ernährungsstatus (NRS-2002-Score ≥3) unterschied sich signifikant zwischen SG und beiden CG (SG: 5/61, CG I: 1/78, CG II: 0/55). Diese Unterschiede konnten jedoch anhand des BMI nicht bestätigt werden.
Schlussfolgerung: Wie erwartet, werden aufgrund der Akute-Phase-Reaktion bei periprothetischen Infektionen (PPI) niedrigere Albumin- und Gesamtproteingehalte beobachtet. Mittels NRS kann ein Ernährungsmangel ausgeschlossen werden, dessen Beurteilung aufgrund des BMI nicht sicher möglich ist. Bei Auftreten einer periprothetischen Gelenkinfektion ist es sinnvoll, den Nährstoffmangel durch Nahrungsergänzungsmittel auszugleichen.
Keywords: Arthroplasty; Body mass index; Malnutrition; Protein deficiency; Vitamin deficiency.
Conflict of interest statement
D. Zajonz, A. Daikos, F. Prager, M. Edel, R. Möbius, J.K. M. Fakler, A. Roth and M. Ghanem declare that they have no competing interests.
Figures
Similar articles
-
The significance of the vitamin D metabolism in the development of periprosthetic infections after THA and TKA: a prospective matched-pair analysis of 240 patients.Clin Interv Aging. 2018 Aug 17;13:1429-1435. doi: 10.2147/CIA.S171307. eCollection 2018. Clin Interv Aging. 2018. PMID: 30147306 Free PMC article.
-
Is potential malnutrition associated with septic failure and acute infection after revision total joint arthroplasty?Clin Orthop Relat Res. 2015 Jan;473(1):175-82. doi: 10.1007/s11999-014-3685-8. Clin Orthop Relat Res. 2015. PMID: 24867449 Free PMC article.
-
Periprosthetic joint infection in aseptic total hip arthroplasty revision.Int Orthop. 2020 Apr;44(4):735-741. doi: 10.1007/s00264-019-04366-2. Epub 2019 Jun 25. Int Orthop. 2020. PMID: 31240360
-
Preoperative Opioid Use Is Associated With Higher Revision Rates in Total Joint Arthroplasty: A Systematic Review.J Arthroplasty. 2021 Nov;36(11):3814-3821. doi: 10.1016/j.arth.2021.06.017. Epub 2021 Jun 24. J Arthroplasty. 2021. PMID: 34247870
-
Correlation between body mass index and two-stage revision failure of periprosthetic joint infection following total joint arthroplasty: A systematic review and meta-analysis.J Orthop Surg (Hong Kong). 2021 Sep-Dec;29(3):23094990211055231. doi: 10.1177/23094990211055231. J Orthop Surg (Hong Kong). 2021. PMID: 34913757
Cited by
-
Preoperative prognostic nutritional index is useful factor for predicting postoperative delirium after primary total joint arthroplasty.BMC Musculoskelet Disord. 2021 Sep 12;22(1):778. doi: 10.1186/s12891-021-04626-6. BMC Musculoskelet Disord. 2021. PMID: 34511076 Free PMC article.
-
Preoperative Risk Factors for Periprosthetic Joint Infection: A Narrative Review of the Literature.Healthcare (Basel). 2024 Mar 15;12(6):666. doi: 10.3390/healthcare12060666. Healthcare (Basel). 2024. PMID: 38540630 Free PMC article. Review.
-
Preoperative strategies to prevent periprosthetic joint infection after knee replacement: evidence-based recommendations for multidisciplinary practice.Orthop Rev (Pavia). 2025 Aug 29;17:143566. doi: 10.52965/001c.143566. eCollection 2025. Orthop Rev (Pavia). 2025. PMID: 40894246 Free PMC article.
-
Moderate-to-Severe Malnutrition Identified by the Controlling Nutritional Status (CONUT) Score Is Significantly Associated with Treatment Failure of Periprosthetic Joint Infection.Nutrients. 2022 Oct 21;14(20):4433. doi: 10.3390/nu14204433. Nutrients. 2022. PMID: 36297116 Free PMC article.
References
-
- Hanssen AD, Osmon DR, Nelson CL. Prevention of deep periprosthetic joint infection. Instr Course Lect. 1997;46:555–567. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials
