

Thromboembolic and bleeding complications in patients with oesophageal cancer
- PMID: 32424862
- PMCID: PMC7497123
- DOI: 10.1002/bjs.11665
Thromboembolic and bleeding complications in patients with oesophageal cancer
Abstract
Background: In patients who undergo curative treatment for oesophageal cancer, risk estimates of venous thromboembolism (VTE), arterial thromboembolism and bleeding are needed to guide decisions about thromboprophylaxis.
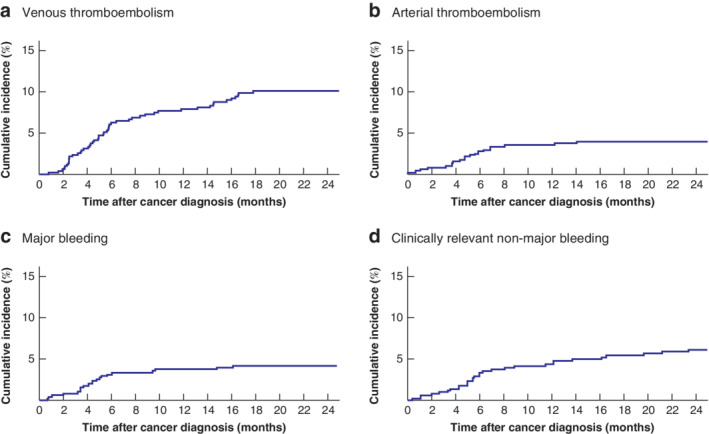
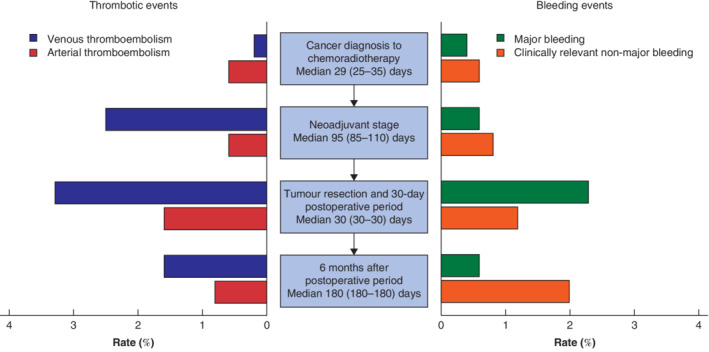
Methods: This was a single-centre, retrospective cohort study of patients with stage I-III oesophageal cancer who received neoadjuvant chemoradiation followed by oesophagectomy. The outcomes VTE, arterial thromboembolism, major bleeding, clinically relevant non-major bleeding and mortality were analysed for four consecutive cancer treatment stages (from diagnosis to neoadjuvant chemoradiotherapy, during neoadjuvant treatment, 30-day postoperative period, and up to 6 months after postoperative period).
Results: Some 511 patients were included. The 2-year survival rate was 67·3 (95 per cent c.i. 63·2 to 71·7) per cent. During the 2-year follow-up, 50 patients (9·8 per cent) developed VTE, 20 (3·9 per cent) arterial thromboembolism, 21 (4·1 per cent) major bleeding and 30 (5·9 per cent) clinically relevant non-major bleeding. The risk of these events was substantial at all treatment stages. Despite 30-day postoperative thromboprophylaxis, 17 patients (3·3 per cent) developed VTE after surgery. Patients with VTE had worse survival (time-varying hazard ratio 1·81, 95 per cent c.i. 1·25 to 2·64). Most bleeding events occurred around the time of medical intervention, and approximately one-half during concomitant use of prophylactic or therapeutic anticoagulation.
Conclusion: Patients with oesophageal cancer undergoing neoadjuvant chemoradiotherapy and surgery are at substantial risk of thromboembolic and bleeding events throughout all stages of treatment. Survival is worse in patients with thromboembolic events during follow-up.
Antecedentes: Para tomar decisiones en cuanto a la profilaxis tromboembólica, es preciso estimar el riesgo de tromboembolismo venoso (venous thromboembolism, VTE), de tromboembolismo arterial y de hemorragia en pacientes a los que se vaya a realizar un tratamiento curativo para el cáncer de esófago. MÉTODOS: Se realizó un estudio de cohortes retrospectivo de un solo centro, de pacientes con cáncer de esófago en estadios I-III que fueron tratados con quimiorradioterapia neoadyuvante y esofagectomía. Se analizaron, en cuatro momentos del tratamiento (desde el momento del diagnóstico hasta la quimiorradioterapia neoadyuvante, durante el tratamiento neoadyuvante, en los 30 días del período postoperatorio y a los 6 meses de la cirugía) las siguientes variables: VTE, tromboembolismo arterial, hemorragia grave, hemorragia no grave clínicamente relevante y mortalidad.
Resultados: Se incluyeron 511 pacientes. La supervivencia a los 2 años fue del 67,3% (ic. del 95%, 63,2-71,7). Durante el seguimiento de 2 años, 50 pacientes desarrollaron un VTE (9,8%), 20 un tromboembolismo arterial (3,9%), 21 hemorragias graves (4,1%) y 30 hemorragias no graves clínicamente relevantes (5,9%). El riesgo de estos accidentes fue notable en todas las etapas del tratamiento. A pesar de la profilaxis tromboembólica posquirúrgica, a los 30 días, 17 pacientes (3,3%) desarrollaron un VTE después de la operación. Los pacientes con VTE tuvieron una supervivencia menor (cociente de riesgos instantáneos, hazard ratio en función del tiempo 1,81; i.c. del 95%, 1,25-2,64). La mayoría de los accidentes hemorrágicos ocurrieron en el contexto de una intervención médica y el 48% durante el uso concomitante de anticoagulación profiláctica o terapéutica. CONCLUSIÓN: Los pacientes con cáncer de esófago tratados con quimiorradioterapia neoadyuvante y cirugía tienen un riesgo sustancial de sufrir accidentes tromboembólicos y hemorrágicos en todas las fases del tratamiento. La supervivencia es peor en aquellos pacientes que presentan accidentes tromboembólicos durante el seguimiento.
© 2020 The Authors. British Journal of Surgery published by John Wiley & Sons Ltd on behalf of BJS Society Ltd.
Figures
Similar articles
-
Outcome of neoadjuvant therapies for cancer of the oesophagus or gastro-oesophageal junction based on a national data registry.Br J Surg. 2016 Dec;103(13):1864-1873. doi: 10.1002/bjs.10304. Epub 2016 Sep 30. Br J Surg. 2016. PMID: 27689845
-
Neoadjuvant chemoradiotherapy or chemotherapy alone for oesophageal cancer: population-based cohort study.Br J Surg. 2021 Apr 30;108(4):403-411. doi: 10.1093/bjs/znaa121. Br J Surg. 2021. PMID: 33755097
-
Conditional survival after neoadjuvant chemoradiotherapy and surgery for oesophageal cancer.Br J Surg. 2020 Jul;107(8):1053-1061. doi: 10.1002/bjs.11476. Epub 2020 Feb 3. Br J Surg. 2020. PMID: 32017047 Free PMC article.
-
[Therapeutic decisions in patients with operable, non-metastatic oesophageal cancer].Zentralbl Chir. 2014 Feb;139(1):32-6. doi: 10.1055/s-0033-1360295. Epub 2014 Feb 28. Zentralbl Chir. 2014. PMID: 24585195 Review. German.
-
Meta-analysis of postoperative morbidity and perioperative mortality in patients receiving neoadjuvant chemotherapy or chemoradiotherapy for resectable oesophageal and gastro-oesophageal junctional cancers.Br J Surg. 2014 Mar;101(4):321-38. doi: 10.1002/bjs.9418. Epub 2014 Feb 3. Br J Surg. 2014. PMID: 24493117 Review.
Cited by
-
Comment On: The Duration and Magnitude of Postdischarge Venous Thromboembolism Following Colectomy.Ann Surg Open. 2022 Nov 2;3(4):e220. doi: 10.1097/AS9.0000000000000220. eCollection 2022 Dec. Ann Surg Open. 2022. PMID: 37600281 Free PMC article. No abstract available.
-
A prospective multicenter study to evaluate the impact of cryotherapy on dysphagia and quality of life in patients with inoperable esophageal cancer.Endoscopy. 2023 Oct;55(10):889-897. doi: 10.1055/a-2105-2177. Epub 2023 Jun 2. Endoscopy. 2023. PMID: 37268010 Free PMC article. Clinical Trial.
References
-
- Falanga A, Marchetti M, Vignoli A. Coagulation and cancer: biological and clinical aspects. J Thromb Haemost 2013; 11: 223–233. - PubMed
-
- Khorana AA, Francis CW, Culakova E, Kuderer NM, Lyman GH. Thromboembolism is a leading cause of death in cancer patients receiving outpatient chemotherapy. J Thromb Haemost 2007; 5: 632–634. - PubMed
-
- Lloyd AJ, Dewilde S, Noble S, Reimer E, Lee AYY. What impact does venous thromboembolism and bleeding have on cancer patients' quality of life? Value Health 2018; 21: 449–455. - PubMed
-
- Bosch DJ, Van Dalfsen QA, Mul VEM, Hospers GAP, Plukker JTM. Increased risk of thromboembolism in esophageal cancer patients treated with neoadjuvant chemoradiotherapy. Am J Surg 2014; 208: 215–221. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
