Real-life assessment of chronic rhinosinusitis patients using mobile technology: The mySinusitisCoach project by EUFOREA
- PMID: 32424899
- PMCID: PMC7687134
- DOI: 10.1111/all.14408
Real-life assessment of chronic rhinosinusitis patients using mobile technology: The mySinusitisCoach project by EUFOREA
Abstract
Background: Chronic rhinosinusitis (CRS) is a chronic inflammatory disease associated with a substantial personal and socioeconomic burden. Monitoring of patient-reported outcomes by mobile technology offers the possibility to better understand real-life burden of CRS.
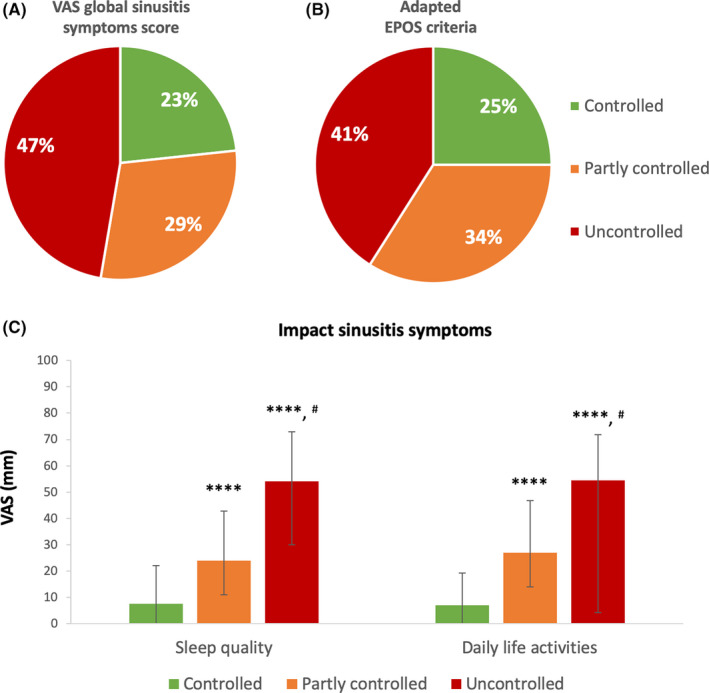
Methods: This study reports on the cross-sectional evaluation of data of 626 users of mySinusitisCoach (mSC), a mobile application for CRS patients. Patient characteristics of mSC users were analysed as well as the level of disease control based on VAS global rhinosinusitis symptom score and adapted EPOS criteria.
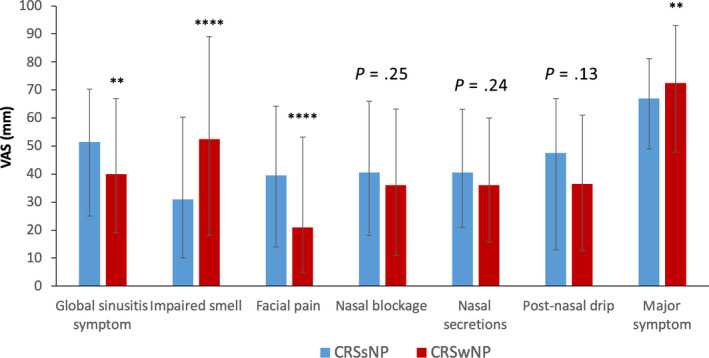
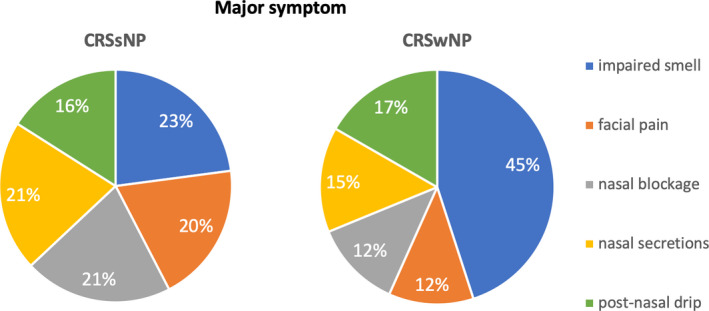
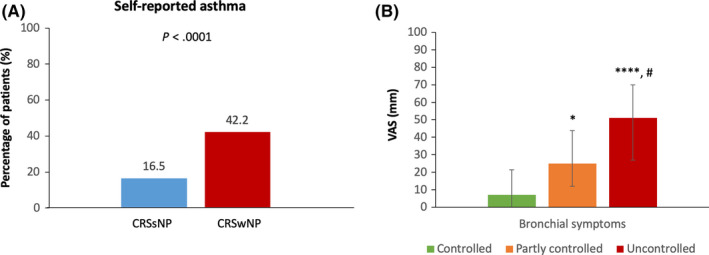
Results: The mSC cohort represents a heterogeneous group of CRS patients with a diverse pattern of major symptoms. Approximately half of patients reported nasal polyps. 47.3% of all CRS patients were uncontrolled based on evaluation of VAS global rhinosinusitis symptom score compared to 40.9% based on adapted EPOS criteria. The impact of CRS on sleep quality and daily life activities was significantly higher in uncontrolled versus well-controlled patients. Half of patients had a history of FESS (functional endoscopic sinus surgery) and reported lower symptom severity compared to patients without a history of FESS, except for patients with a history of more than 3 procedures. Patients with a history of FESS reported higher VAS levels for impaired smell.
Conclusion: Real-life data confirm the high disease burden in uncontrolled CRS patients, clearly impacting quality of life. Sinus surgery improves patient-reported outcomes, but not in patients with a history of more than 3 procedures. Mobile technology opens a new era of real-life monitoring, supporting the evolution of care towards precision medicine.
Keywords: Mobile health technology; nasal polyp; patient-reported outcome measure; real-world evidence; visual analogue scale.
© 2020 The Authors. Allergy published by European Academy of Allergy and Clinical Immunology and John Wiley & Sons Ltd.
Conflict of interest statement
Dr Alobid reports personal fees from Roche, personal fees from Menarini, personal fees from Mylan, personal fees from Novartis, personal fees from MSD, outside the submitted work. Dr Bachert reports personal fees from Sanofi, GSK, AstraZeneca and Novartis and grants and personal fees from Mylan, outside the submitted work. Dr Bernal‐Sprekelsen has nothing to disclose. Dr Bjermer is member of the Board of EUFOREA that owns the mySinusitisCoach application. Dr Callebaut has nothing to disclose. Dr Cardell reports grants from Sanofi, outside the submitted work. Dr Carrie has nothing to disclose. Dr Castelnuovo has nothing to disclose. Dr Cathcart has nothing to disclose. Dr Clement has nothing to disclose. Dr Constantinidis has nothing to disclose. Ms Cools has nothing to disclose. Dr Cornet has nothing to disclose. Dr Cox has nothing to disclose. Dr Correia‐de‐Sousa reports other from Boheringer Ingelheim, grants, personal fees and other from GSK, grants and other from AstraZeneca, personal fees from Mundipharma, outside the submitted work. Dr De Bont has nothing to disclose. Ms Deneyer is employed by Change Accelerator in Respiratory Diseases. Dr Delsupehe has nothing to disclose. Dr Devos has nothing to disclose. Dr Doulaptsi has nothing to disclose. Dr Fokkens reports that the Amsterdam University Medical Centres, location AMC receives grants and Stichting AERO receives personal fees from Sanofi and Novartis, grants from Gsk, from Meda, from ALK, from Allergy therapeutics, outside the submitted work. Dr Gane has nothing to disclose. Dr Gevaert has nothing to disclose. Dr Hellings reports personal fees from Sanofi, personal fees from Allergopharma, personal fees from Stallergenes, grants and personal fees from Mylan, outside the submitted work. He is also member of the Board of EUFOREA that owns the mySinusitisCoach application. Dr Hopkins has nothing to disclose. Dr Hox reports personal fees from Consultant work for ALK, outside the submitted work. Dr Hummel reports grants from Sony, Stuttgart, Germany, grants from Smell and Taste Lab, Geneva, Switzerland, grants from Takasago, Paris, France, grants from aspuraclip, Berlin, Germany, outside the submitted work. Dr Hosemann has nothing to disclose. Dr Jacobs has nothing to disclose. Dr Jorissen has nothing to disclose. Dr Kjeldsen reports other from Astra Zeneca, outside the submitted work. Dr Landis has nothing to disclose. Dr Lemmens has nothing to disclose. Dr Leunig has nothing to disclose. Dr Lund has nothing to disclose. Mr Mariën is employed by Change Accelerator in Respiratory Diseases and advisor to EUFOREA. Dr Mullol reports personal fees and other from SANOFI‐GENZYME & REGENERON, NOVARTIS and ALLAKOS, grants and personal fees from MYLAN Pharma and URIACH Group, personal fees from Mitsubishi‐Tanabe, Menarini, UCB, AstraZeneca, GSK and MSD, outside the submitted work. Dr Onerci has nothing to disclose. Mrs Palkonen has nothing to disclose. Mrs Proano has nothing to disclose. Dr Prokopakis has nothing to disclose. Dr Pugin has nothing to disclose. Dr Ryan reports personal fees and non‐financial support from Mylan, personal fees from Chiesi, personal fees from GSK, personal fees from Novartis, personal fees from Regeneron, personal fees from BI, outside the submitted work. Dr Riechelmann has nothing to disclose. Dr Sahlstrand Johnson reports grants and personal fees from Medtronic, outside the submitted work. Dr Toppila‐Salmi reports personal fees from ERT, Roche products, Sanofi Pharma and Novartis, grants from GSK, outside the submitted work. Dr Segboer has nothing to disclose. Dr Seys is employed by Change Accelerator in Respiratory Diseases. Dr Speleman has nothing to disclose. Dr Steinsvik has nothing to disclose. Dr Surda has nothing to disclose. Dr Tomazic has nothing to disclose. Dr Vanderveken has nothing to disclose. Dr Van Gerven has nothing to disclose. Dr Van Zele has nothing to disclose. Dr Verfaillie has nothing to disclose. Dr Verhaeghe has nothing to disclose. Dr Vierstraete has nothing to disclose. Dr Vlaminck has nothing to disclose. Dr Wagenmann reports personal fees from ALK‐Abelló, Allergopharma, AstraZeneca, Bencard Allergie, Genzyme, HAL Allergie, Infectopharm, LETI Pharma, MEDA Pharma, Novartis, Sanofi Aventis, Stallergenes and Teva, outside the submitted work.
Figures