

Cardiovascular Implications of the COVID-19 Pandemic: A Global Perspective
- PMID: 32425328
- PMCID: PMC7229739
- DOI: 10.1016/j.cjca.2020.05.018
Cardiovascular Implications of the COVID-19 Pandemic: A Global Perspective
Abstract
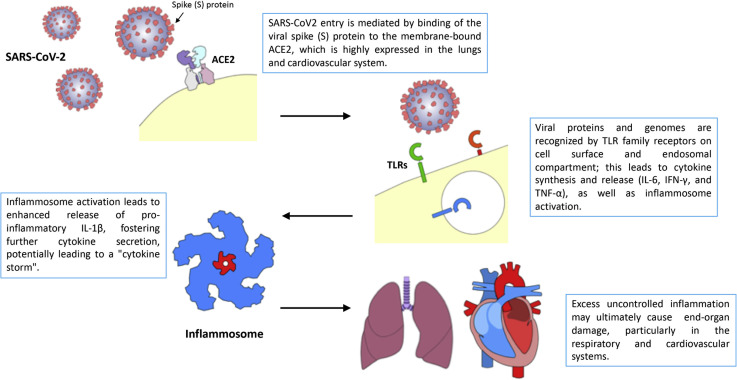
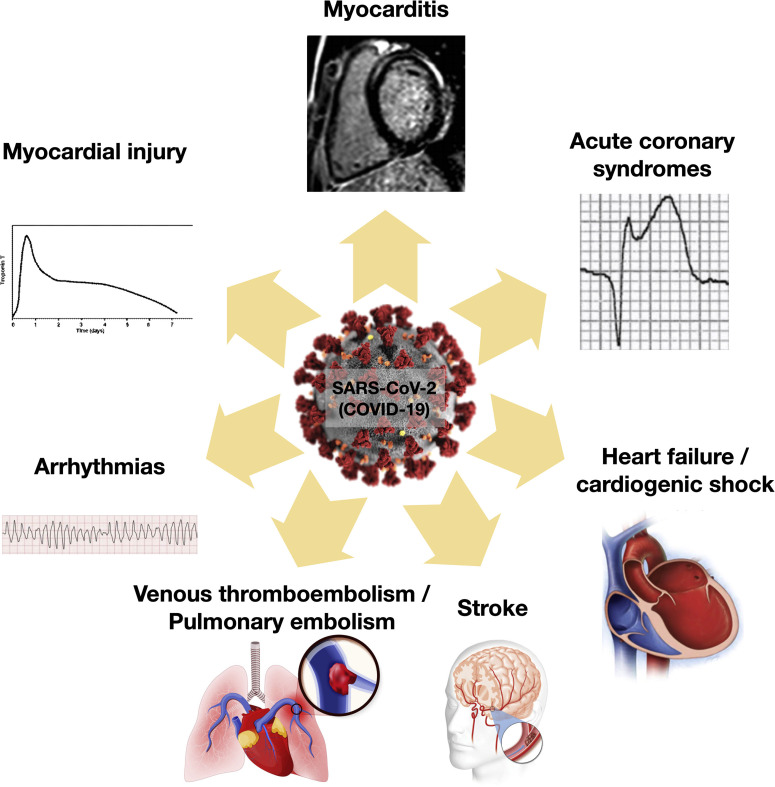
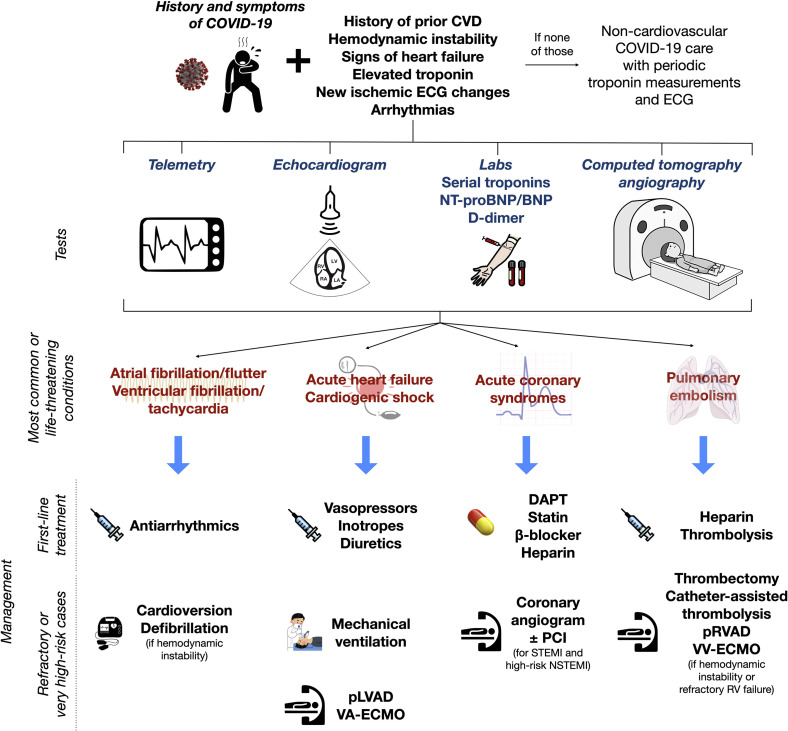
The coronavirus disease 2019 (COVID-19), caused by severe acute respiratory syndrome coronavirus-2 (SARS-CoV-2), represents the pandemic of the century, with approximately 3.5 million cases and 250,000 deaths worldwide as of May 2020. Although respiratory symptoms usually dominate the clinical presentation, COVID-19 is now known to also have potentially serious cardiovascular consequences, including myocardial injury, myocarditis, acute coronary syndromes, pulmonary embolism, stroke, arrhythmias, heart failure, and cardiogenic shock. The cardiac manifestations of COVID-19 might be related to the adrenergic drive, systemic inflammatory milieu and cytokine-release syndrome caused by SARS-CoV-2, direct viral infection of myocardial and endothelial cells, hypoxia due to respiratory failure, electrolytic imbalances, fluid overload, and side effects of certain COVID-19 medications. COVID-19 has profoundly reshaped usual care of both ambulatory and acute cardiac patients, by leading to the cancellation of elective procedures and by reducing the efficiency of existing pathways of urgent care, respectively. Decreased use of health care services for acute conditions by non-COVID-19 patients has also been reported and attributed to concerns about acquiring in-hospital infection. Innovative approaches that leverage modern technologies to tackle the COVID-19 pandemic have been introduced, which include telemedicine, dissemination of educational material over social media, smartphone apps for case tracking, and artificial intelligence for pandemic modelling, among others. This article provides a comprehensive overview of the pathophysiology and cardiovascular implications of COVID-19, its impact on existing pathways of care, the role of modern technologies to tackle the pandemic, and a proposal of novel management algorithms for the most common acute cardiac conditions.
La maladie à coronavirus 2019 (COVID-19), causée par le SARS-CoV-2 (severe acute respiratory syndrome coronarivus-2 pour coronavirus du syndrome respiratoire aigu sévère 2), est la pandémie du siècle; en mai 2020, on dénombrait quelque 3,5 millions de cas et 250 000 décès dans le monde. Bien que les symptômes respiratoires dominent généralement le tableau clinique, on sait maintenant que la COVID-19 peut aussi avoir de graves conséquences sur le plan cardiovasculaire, par exemple des lésions myocardiques, des myocardites, des syndromes coronariens aigus, des embolies pulmonaires, des accidents vasculaires cérébraux, des arythmies, des insuffisances cardiaques et des chocs cardiogéniques. Les manifestations cardiaques de la COVID-19 pourraient être liées à la stimulation adrénergique, à l’inflammation généralisée et au syndrome de libération des cytokines causés par le SARS-CoV-2, à l’infection directe des cellules myocardiques et endothéliales par le virus, à l’hypoxie provoquée par l’insuffisance respiratoire, à un déséquilibre électrolytique, à une surcharge liquidienne et aux effets indésirables de certains médicaments utilisés pour traiter les symptômes de la COVID-19. En forçant l’annulation des interventions non urgentes et en réduisant l’efficacité des voies d’accès aux soins d’urgence, la COVID-19 a profondément transformé les soins usuels prodigués à tous les patients en cardiologie, qu’ils aient besoin de soins ambulatoires ou aigus. On a aussi observé une diminution de l’utilisation de services de soins de santé pour des problèmes aigus par les patients non atteints de COVID-19, une situation attribuée à la crainte de contracter le virus à l’hôpital. Des approches novatrices faisant appel aux technologies modernes ont été mises en œuvre pour pallier les restrictions imposées par la pandémie de COVID-19, entre autres : télémédecine, diffusion de matériel éducatif dans les médias sociaux, suivi des cas au moyen d’applications pour téléphone intelligent et modélisation de la pandémie grâce à l’intelligence artificielle. Les auteurs de cet article passent en revue les conséquences de la COVID-19 sur les plans physiopathologique et cardiovasculaire, ses répercussions sur les voies d’accès aux soins actuelles et le rôle des technologies modernes dans la lutte contre la pandémie, et proposent de nouveaux algorithmes de prise en charge des problèmes de santé cardiaque aigus les plus courants.
Copyright © 2020 Canadian Cardiovascular Society. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Johns Hopkins University COVID-19 Resource Center. www.worldometers.info/coronavirus/countries-where-coronavirus-has-spread Available at.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Miscellaneous
