

Evidence Supporting a Phased Immuno-physiological Approach to COVID-19 From Prevention Through Recovery
- PMID: 32425712
- PMCID: PMC7190003
Evidence Supporting a Phased Immuno-physiological Approach to COVID-19 From Prevention Through Recovery
Abstract
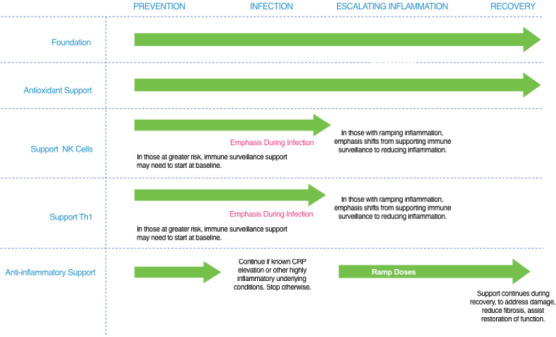
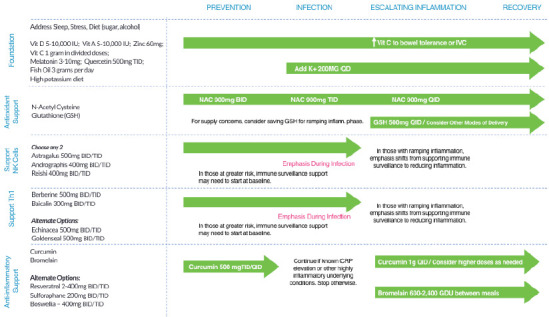
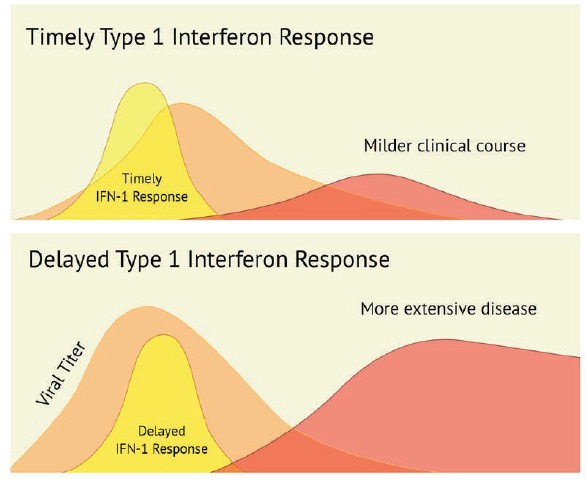
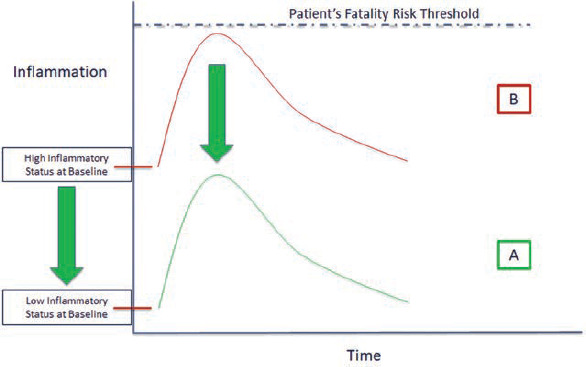
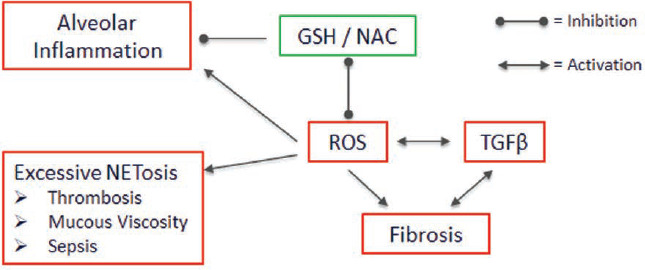
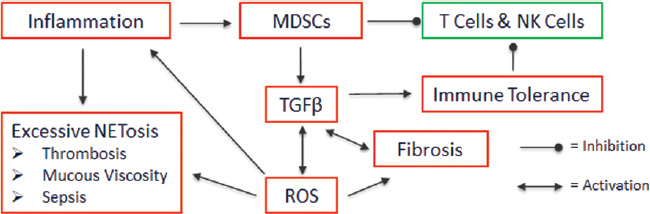
This paper presents an evidence-based strategy for improving clinical outcomes in COVID-19. Recommendations are based on the phases of the disease, because optimal interventions for one phase may not be appropriate for a different phase. The four phases addressed are: Prevention, Infection, Inflammation and Recovery. Underlying this phased approach is recognition of emerging evidence for two different components of pathophysiology, early infection and late stage severe complications. These two aspects of the disease suggest two different patterns of clinical emphasis that seem on the surface to be not entirely concordant. We describe the application of therapeutic strategies and appropriate tactics that address four main stages of disease progression for COVID-19. Emerging evidence in COVID-19 suggests that the SARS-CoV-2 virus may both evade the innate immune response and kill macrophages. Delayed innate immune response and a depleted population of macrophages can theoretically result in a blunted antigen presentation, delaying and diminishing activation of the adaptive immune response. Thus, one clinical strategy involves supporting patient innate and adaptive immune responses early in the time course of illness, with the goal of improving the timeliness, readiness, and robustness of both the innate and adaptive immune responses. At the other end of the disease pathology spectrum, risk of fatality in COVID-19 is driven by excessive and persistent upregulation of inflammatory mechanisms associated with cytokine storm. Thus, the second clinical strategy is to prevent or mitigate excessive inflammatory response to prevent the cytokine storm associated with high mortality risk. Clinical support for immune system pathogen clearance mechanisms involves obligate activation of immune response components that are inherently inflammatory. This puts the goals of the first clinical strategy (immune activation) potentially at odds with the goals of the second strategy(mitigation of proinflammatory effects). This creates a need for discernment about the time course of the illness and with that, understanding of which components of an overall strategy to apply at each phase of the time course of the illness. We review evidence from early observational studies and the existing literature on both outcomes and mechanisms of disease, to inform a phased approach to support the patient at risk for infection, with infection, with escalating inflammation during infection, and at risk of negative sequelae as they move into recovery.
Copyright © 2020 InnoVision Health Media Inc.
Figures
References
-
- Prompetchara E, Ketloy C, Palaga T. Immune responses in COVID-19 and potential vaccines: Lessons learned from SARS and MERS epidemic. Asian Pac J Allergy Immunol. 2020. March;38(1):1-9. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous