

Healing Status of Meniscal Ramp Lesion Affects Anterior Knee Stability After ACL Reconstruction
- PMID: 32426412
- PMCID: PMC7222250
- DOI: 10.1177/2325967120917674
Healing Status of Meniscal Ramp Lesion Affects Anterior Knee Stability After ACL Reconstruction
Abstract
Background: Although the biomechanical importance of the ramp lesion in the anterior cruciate ligament (ACL)-deficient knee has been demonstrated, there is no clear consensus on the appropriate treatment for ramp lesions during ACL reconstruction.
Purpose: To compare the postoperative outcomes for ramp lesions between patients treated with all-inside repair through the posteromedial portal and those whose ramp lesions were left in situ without repair during ACL reconstruction. We also determined whether ramp lesion healing status affected postoperative knee stability.
Study design: Cohort study; Level of evidence, 3.
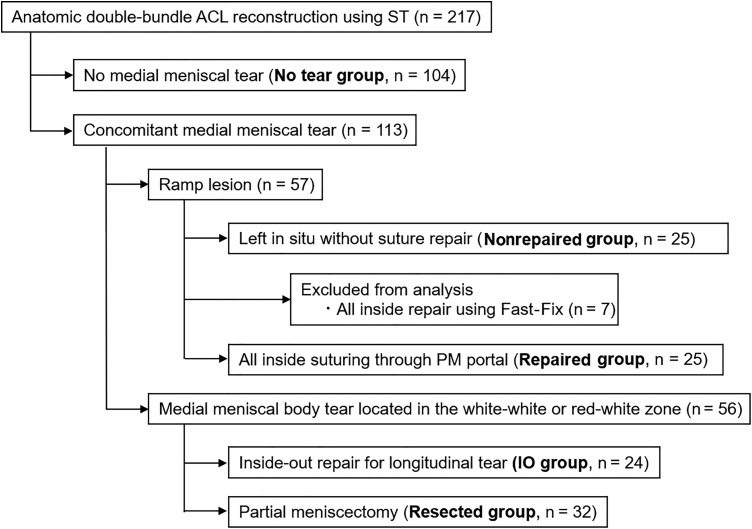
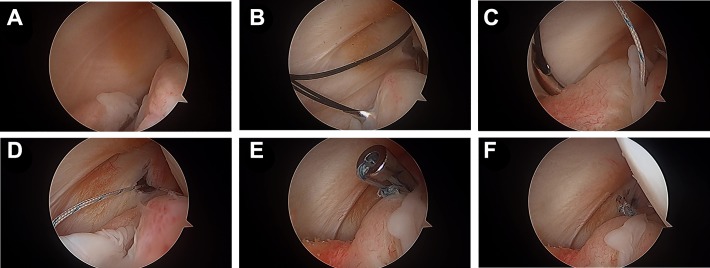
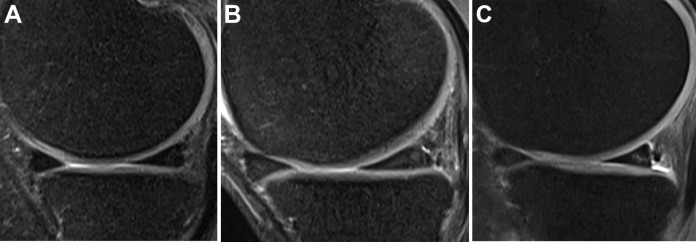
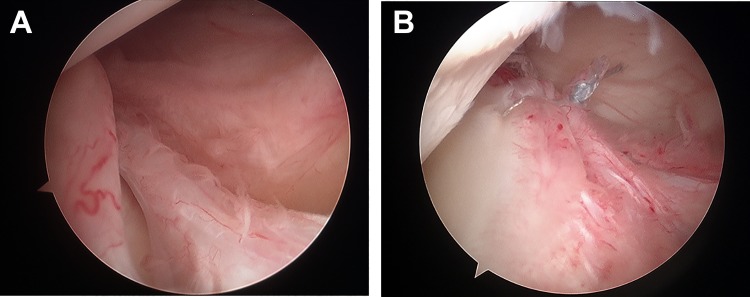
Methods: A total of 57 patients who underwent anatomic double-bundle ACL reconstruction between August 2011 and December 2017 had attendant ramp lesions. Of these, 25 ramp lesions that were considered stable were left in situ without repair (Nonrepaired group), and 25 ramp lesions, including 21 stable and 4 unstable lesions, were treated using all-inside repair through the posteromedial portal (Repaired group). We evaluated the side-to-side difference (SSD) in anterior tibial translation on stress radiographs and rotational stability by using the pivot-shift test 2 years after surgery, and healing status of the ramp lesions was evaluated on 3.0-T magnetic resonance imaging (MRI) scans 1 year after surgery.
Results: The mean SSDs in anterior translation were 2.4 ± 1.6 mm for the Nonrepaired group and 1.9 ± 1.6 mm for the Repaired group, with no significant differences. The positive ratios on the pivot-shift test were not significantly different between groups. Healing rates of ramp lesions on MRI scans showed a significant difference between the Nonrepaired group (60%) and the Repaired group (100%) (P = .001). The mean SSDs for knees in which the ramp lesion had healed as shown on MRI scans and those in which it had not healed were 1.9 ± 1.6 mm and 3.2 ± 1.1 mm, respectively, which was a significant difference (P = .02).
Conclusion: Healing rates of ramp lesions were significantly better in the Repaired group than in the Nonrepaired group, although postoperative knee stability was not significantly different between groups. Anterior laxity in the knees in which the ramp lesion was unhealed was significantly greater compared with the knees in which the ramp lesion healed. All-inside repair through the posteromedial portal was a reliable surgical procedure to heal ramp lesions.
Keywords: anterior cruciate ligament; anterior stability; ramp lesion; repair.
© The Author(s) 2020.
Conflict of interest statement
The authors declared that there are no conflicts of interest in the authorship and publication of this contribution. AOSSM checks author disclosures against the Open Payments Database (OPD). AOSSM has not conducted an independent investigation on the OPD and disclaims any liability or responsibility relating thereto.
Figures
Similar articles
-
Is It Necessary to Repair Stable Ramp Lesions of the Medial Meniscus During Anterior Cruciate Ligament Reconstruction? A Prospective Randomized Controlled Trial.Am J Sports Med. 2017 Apr;45(5):1004-1011. doi: 10.1177/0363546516682493. Epub 2017 Jan 6. Am J Sports Med. 2017. PMID: 28060534 Clinical Trial.
-
Effect of Meniscocapsular and Meniscotibial Lesions in ACL-Deficient and ACL-Reconstructed Knees: A Biomechanical Study.Am J Sports Med. 2018 Aug;46(10):2422-2431. doi: 10.1177/0363546518774315. Epub 2018 May 30. Am J Sports Med. 2018. PMID: 29847148
-
Posteromedial Meniscocapsular Lesions Increase Tibiofemoral Joint Laxity With Anterior Cruciate Ligament Deficiency, and Their Repair Reduces Laxity.Am J Sports Med. 2016 Feb;44(2):400-8. doi: 10.1177/0363546515617454. Epub 2015 Dec 11. Am J Sports Med. 2016. PMID: 26657852
-
Examining Techniques for Treatment of Medial Meniscal Ramp Lesions During Anterior Cruciate Ligament Reconstruction: A Systematic Review.Arthroscopy. 2020 Nov;36(11):2921-2933. doi: 10.1016/j.arthro.2020.05.041. Epub 2020 Jul 14. Arthroscopy. 2020. PMID: 32674943
-
The fate of unrepaired stable ramp lesions: a systematic review.Acta Orthop Belg. 2024 Sep;90(3):543-548. doi: 10.52628/90.3.11174. Acta Orthop Belg. 2024. PMID: 39851027
Cited by
-
Clinical and MRI Outcomes of Repaired Peripheral Longitudinal Tears of the Posterior Horn of the Medial Meniscus With ACL Reconstruction: Results According to Tear Size.Orthop J Sports Med. 2023 Aug 25;11(8):23259671231167535. doi: 10.1177/23259671231167535. eCollection 2023 Aug. Orthop J Sports Med. 2023. PMID: 37655242 Free PMC article.
-
Searching for the Best Treatment for Ramp Lesions: A Systematic Review and Network Meta-Analysis.Cureus. 2023 Jul 10;15(7):e41651. doi: 10.7759/cureus.41651. eCollection 2023 Jul. Cureus. 2023. PMID: 37435014 Free PMC article. Review.
-
Effect of Ramp Lesions on Outcomes After Anterior Cruciate Ligament Reconstruction.Orthop J Sports Med. 2025 Jan 31;13(1):23259671241308015. doi: 10.1177/23259671241308015. eCollection 2025 Jan. Orthop J Sports Med. 2025. PMID: 39896173 Free PMC article.
-
Greater Knee Rotatory Instability After Posterior Meniscocapsular Injury Versus Anterolateral Ligament Injury: A Proposed Mechanism of High-Grade Pivot Shift.Orthop J Sports Med. 2023 Sep 6;11(9):23259671231188712. doi: 10.1177/23259671231188712. eCollection 2023 Sep. Orthop J Sports Med. 2023. PMID: 37693803 Free PMC article.
-
Short-Term Outcomes After Treatment of Isolated Hidden Meniscal Ramp Lesions.Orthop J Sports Med. 2022 Apr 1;10(4):23259671221085977. doi: 10.1177/23259671221085977. eCollection 2022 Apr. Orthop J Sports Med. 2022. PMID: 35386838 Free PMC article.
References
-
- Ahlden M, Samuelsson K, Sernert N, Forssblad M, Karlsson J, Kartus J. The Swedish National Anterior Cruciate Ligament Register: a report on baseline variables and outcomes of surgery for almost 18,000 patients. Am J Sports Med. 2012;40:2230–2235. - PubMed
-
- Ahn JH, Wang JH, Yoo JC. Arthroscopic all-inside suture repair of medial meniscus lesion in anterior cruciate ligament-deficient knees: results of second-look arthroscopies in 39 cases. Arthroscopy. 2004;20:101–108. - PubMed
-
- Ahn JH, Lee YS, Yoo JC, Chang MJ, Koh KH, Kim MH. Clinical and second-look arthroscopic evaluation of repaired medial meniscus in anterior cruciate ligament-reconstructed knees. Am J Sports Med. 2010;38:472–477. - PubMed
-
- Bollen SR. Posteromedial meniscocapsular injury associated with rupture of the anterior cruciate ligament: a previously unrecognized association. Bone Joint J. 2010;92:222–223. - PubMed
-
- Crues JV III, Ryu R, Morgan FW. Meniscal pathology: the expanding role of magnetic resonance imaging. Clin Orthop Relat Res. 1990;252:80–87. - PubMed
LinkOut - more resources
Full Text Sources
