

Prioritisation of ICU treatments for critically ill patients in a COVID-19 pandemic with scarce resources
- PMID: 32426441
- PMCID: PMC7230138
- DOI: 10.1016/j.accpm.2020.05.008
Prioritisation of ICU treatments for critically ill patients in a COVID-19 pandemic with scarce resources
Abstract
Background: Relying on capacity increases and patient transfers to deal with the huge and continuous inflow of COVID-19 critically ill patients is a strategy limited by finite human and logistical resources.
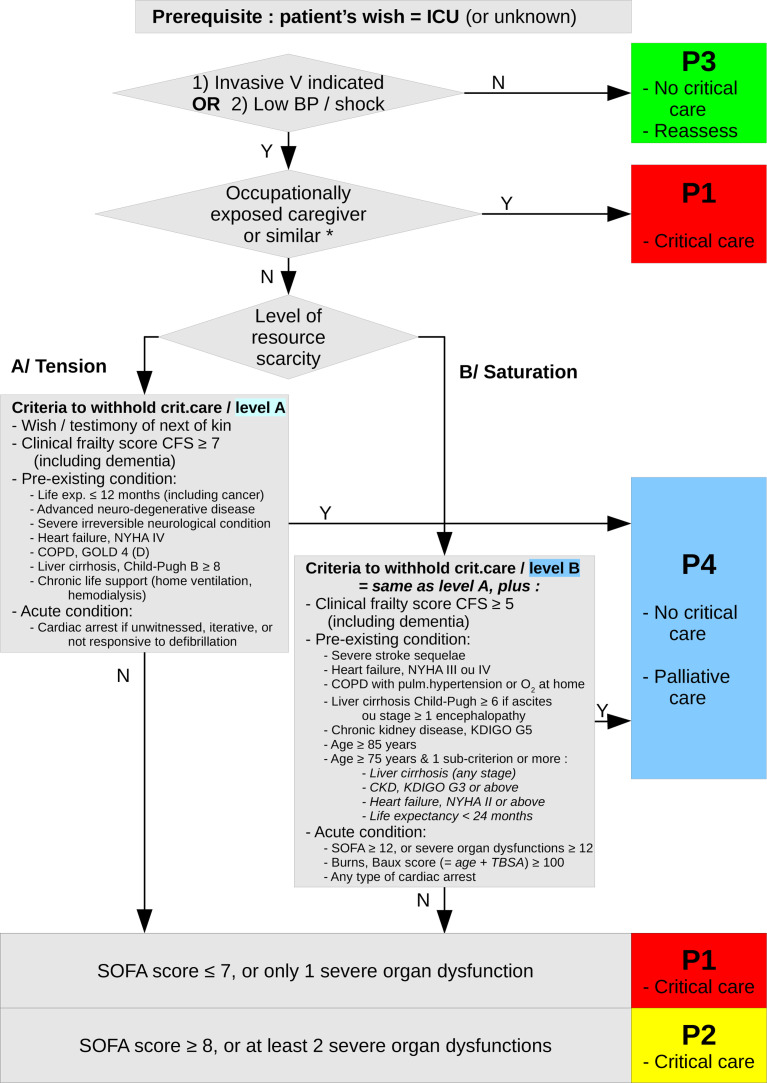
Rationale: Prioritising both critical care initiation and continuation is paramount to save the greatest number of lives. It enables to allocate scarce resources in priority to those with the highest probability of benefiting from them. It is fully ethical provided it relies on objective and widely shared criteria, thus preventing arbitrary decisions and guaranteeing equity. Prioritisation seeks to fairly allocate treatments, maximise saved lives, gain indirect life benefits from prioritising exposed healthcare and similar workers, give priority to those most penalised as a last resort, and apply similar prioritisation schemes to all patients.
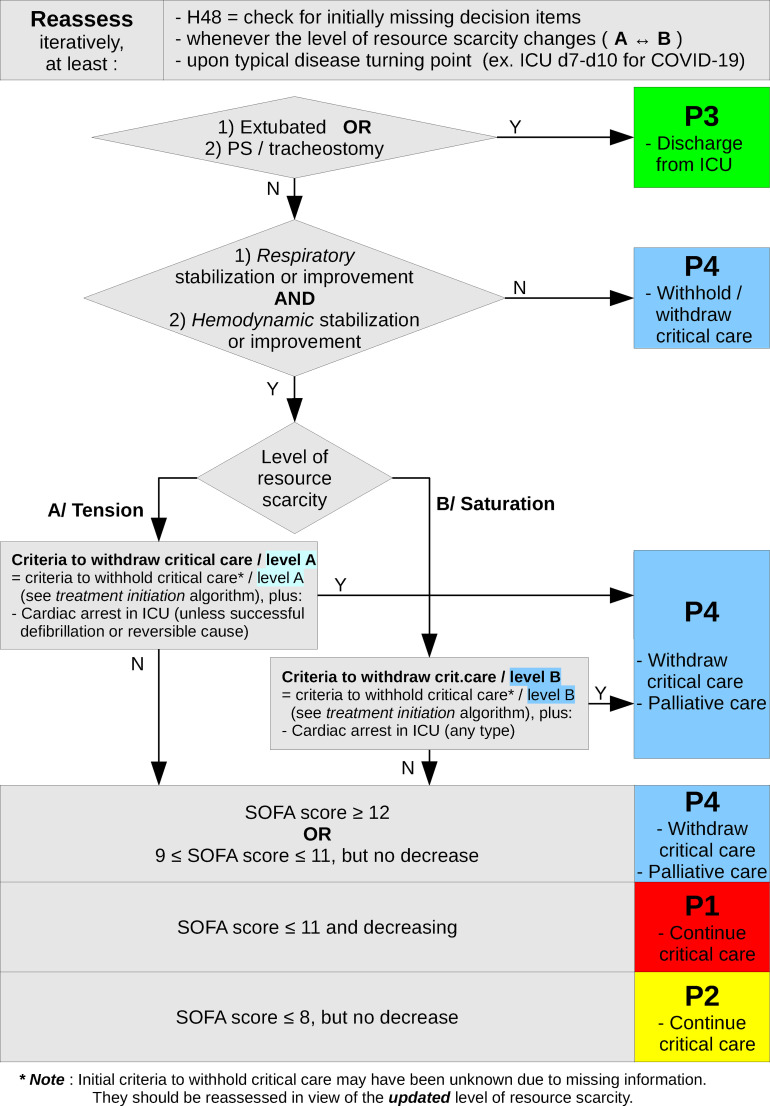
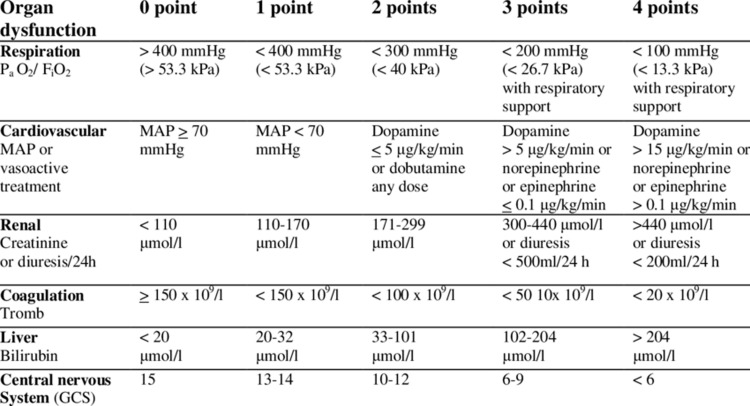
Prioritisation strategy: Prioritisation schemes and their criteria are adjusted to the level of resource scarcity: strain (level A) or saturation (level B). Prioritisation yields a four level priority for initiation or continuation of critical care: P1-high priority, P2-intermediate priority, P3-not needed, P4-not appropriate. Prioritisation schemes take into account the patient's wishes, clinical frailty, pre-existing chronic condition, along with severity and evolution of acute condition. Initial priority level must be reassessed, at least after 48h once missing decision elements are available, at the typical turning point in the disease's natural history (ICU days 7 to 10 for COVID-19), and each time resource scarcity levels change. For treatments to be withheld or withdrawn, a collegial decision-making process and information of patient and/or next of kin are paramount.
Perspective: Prioritisation strategy is bound to evolve with new knowledge and with changes within the epidemiological situation.
Keywords: COVID-19; Critical care; Ethics; Pandemic; Prioritisation; Triage.
Copyright © 2020 Société française d'anesthésie et de réanimation (Sfar). Published by Elsevier Masson SAS. All rights reserved.
Figures
Similar articles
-
COVID-19 and ethical considerations: Valuable decision-making tools from the leading medical societies in France.Anaesth Crit Care Pain Med. 2020 Jun;39(3):365-366. doi: 10.1016/j.accpm.2020.05.001. Epub 2020 May 7. Anaesth Crit Care Pain Med. 2020. PMID: 32414630 Free PMC article. No abstract available.
-
[Ethical guides, criteria for admission in intensive care, palliative care. Multi-society recommendations for allocation of resources during the COVID-19 pandemic].Medicina (B Aires). 2020;80 Suppl 3:45-64. Medicina (B Aires). 2020. PMID: 32658848 Spanish.
-
COVID-19 pandemic: triage for intensive-care treatment under resource scarcity.Swiss Med Wkly. 2020 Mar 24;150:w20229. doi: 10.4414/smw.2020.20229. eCollection 2020 Mar 23. Swiss Med Wkly. 2020. PMID: 32208495 No abstract available.
-
[Ethical recommendations for a difficult decision-making in intensive care units due to the exceptional situation of crisis by the COVID-19 pandemia: A rapid review & consensus of experts].Med Intensiva (Engl Ed). 2020 Oct;44(7):439-445. doi: 10.1016/j.medin.2020.04.006. Epub 2020 Apr 15. Med Intensiva (Engl Ed). 2020. PMID: 32402532 Free PMC article. Review.
-
Practices in Triage and Transfer of Critically Ill Patients: A Qualitative Systematic Review of Selection Criteria.Crit Care Med. 2020 Nov;48(11):e1147-e1157. doi: 10.1097/CCM.0000000000004624. Crit Care Med. 2020. PMID: 32858530 Free PMC article.
Cited by
-
Mental disorders, COVID-19-related life-saving measures and mortality in France: A nationwide cohort study.PLoS Med. 2023 Feb 6;20(2):e1004134. doi: 10.1371/journal.pmed.1004134. eCollection 2023 Feb. PLoS Med. 2023. PMID: 36745669 Free PMC article.
-
Predicting intubation risk among COVID-19 hospitalized patients using artificial neural networks.J Educ Health Promot. 2023 Jan 31;12:16. doi: 10.4103/jehp.jehp_20_22. eCollection 2023. J Educ Health Promot. 2023. PMID: 37034879 Free PMC article.
-
Advanced predictive modeling for enhanced mortality prediction in ICU stroke patients using clinical data.PLoS One. 2025 May 28;20(5):e0323441. doi: 10.1371/journal.pone.0323441. eCollection 2025. PLoS One. 2025. PMID: 40435317 Free PMC article.
-
Ethical factors determining ECMO allocation during the COVID-19 pandemic.BMC Med Ethics. 2021 Jun 1;22(1):70. doi: 10.1186/s12910-021-00638-y. BMC Med Ethics. 2021. PMID: 34074282 Free PMC article.
-
Validation of a pre-established triage protocol for critically ill patients in a COVID-19 outbreak under resource scarcity: A retrospective multicenter cohort study.PLoS One. 2023 May 11;18(5):e0285690. doi: 10.1371/journal.pone.0285690. eCollection 2023. PLoS One. 2023. PMID: 37167306 Free PMC article.
References
-
- Azoulay E., Beloucif S., Vivien B., Guidet B., Pateron D., Le Dorze M. Regional recommendations - ARS; Ile-de-France: 2020. [Decision to admit patients to Intensive care units in COVID-19 pandemic (in French)] [https://www.srlf.org/wp-content/uploads/2020/03/ARS-ETHIQUE-COVID-final.pdf (accessed March 31, 2020)]
-
- Comité consultatif national d’éthique . 2020. Ethical considerations in pandemic (in French) [https://www.ccne-ethique.fr/sites/default/files/reponse_ccne_-_covid-19_... (accessed March 31, 2020)]
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
