

Histopathological lesions and exposure to Plasmodium falciparum infections in the placenta increases the risk of preeclampsia among pregnant women
- PMID: 32427864
- PMCID: PMC7237676
- DOI: 10.1038/s41598-020-64736-4
Histopathological lesions and exposure to Plasmodium falciparum infections in the placenta increases the risk of preeclampsia among pregnant women
Abstract
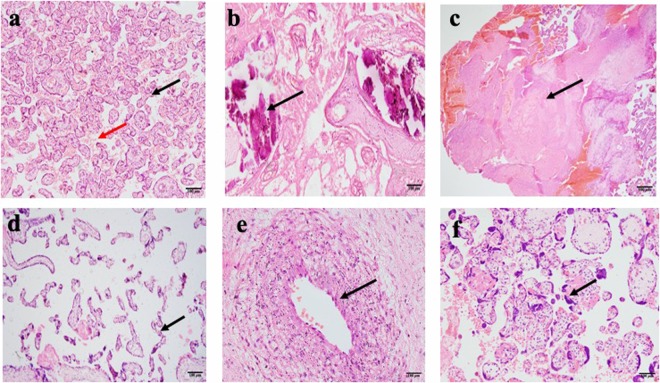
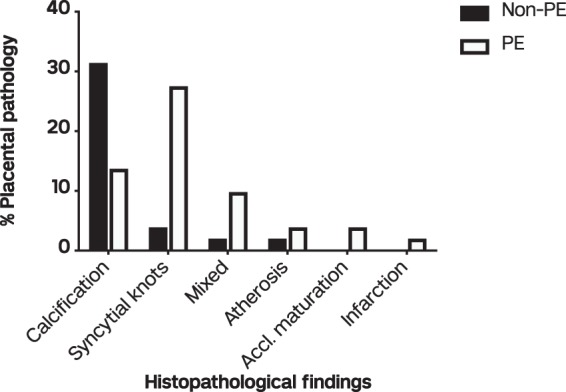
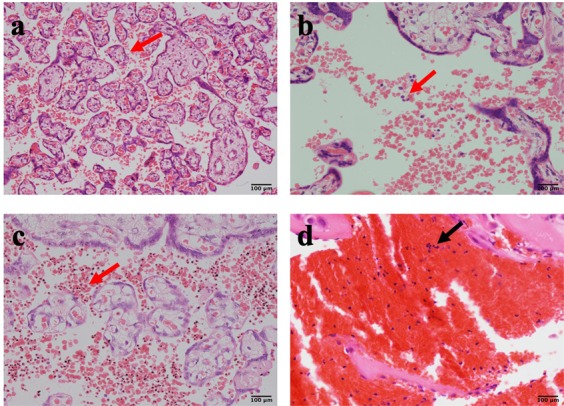
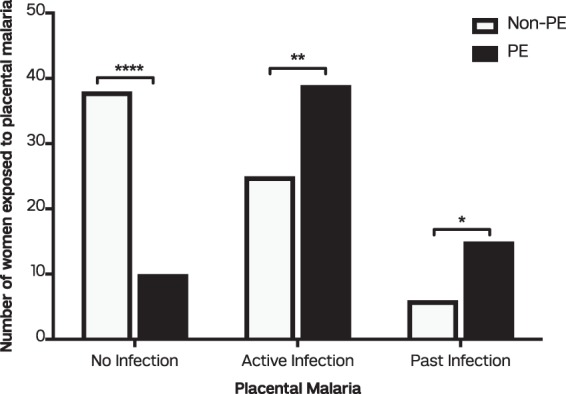
Preeclampsia (PE) is a placental disorder with different phenotypic presentations. In malaria-endemic regions, high incidence of PE is reported, with debilitating foeto-maternal effects, particularly among primigravid women. However, the relationship between placental pathology and Plasmodium falciparum infection in the placenta with PE is underexplored. Placentas from 134 pregnant women were examined after delivery for pathological lesions and placental malaria (PM). They comprised of 69 women without PE (non-PE group) and 65 women diagnosed with PE (PE group). The presence of placental pathology increased the risk of PE, with particular reference to syncytial knots. Placental malaria was 64 (48.1%) and 21 (15.8%) respectively for active and past infections and these proportions were significantly higher in the PE group compared to the non-PE group. Further multivariate analyses showed placental pathology (adjusted (aOR) 3.0, 95% CI = 1.2-7.5), active PM (aOR 6.7, 95% CI = 2.3-19.1), past PM (aOR 12.4, 95% CI = 3.0-51.0) and primigravidity (aOR 6.6, 95% CI 2.4-18.2) to be associated with PE. Our findings suggest that placental histological changes and PM are independent risk factors for PE particularly in primigravida. These findings might improve the management of PE in malaria-endemic regions.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
-
- Tranquilli A, et al. The classification, diagnosis and management of the hypertensive disorders of pregnancy: A revised statement from the ISSHP. Pregnancy. Hypertension: An International Journal of Women’s Cardiovascular Health. 2014;4(2):97–104. - PubMed
-
- Ghana Statistical Service (GSS), G.H.S.G., and ICF. Ghana Maternal Health Survey 2017. Accra: Ghana Demogr Health Surv 2018; Available from: https://dhsprogram.com/pubs/pdf/FR340/FR340.pdf (Accessed: 15th August 2019).
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
