

Imaging Modalities for the Diagnosis of Vascular Graft Infections: A Consensus Paper amongst Different Specialists
- PMID: 32429584
- PMCID: PMC7290746
- DOI: 10.3390/jcm9051510
Imaging Modalities for the Diagnosis of Vascular Graft Infections: A Consensus Paper amongst Different Specialists
Abstract
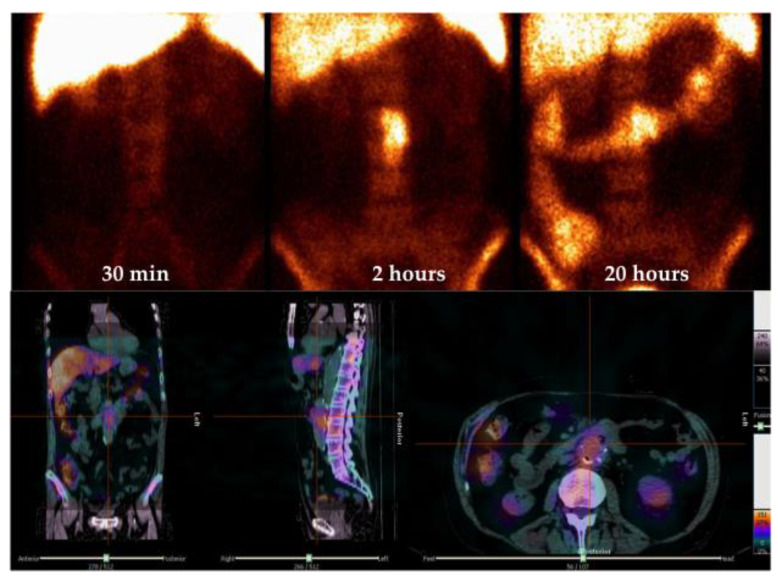
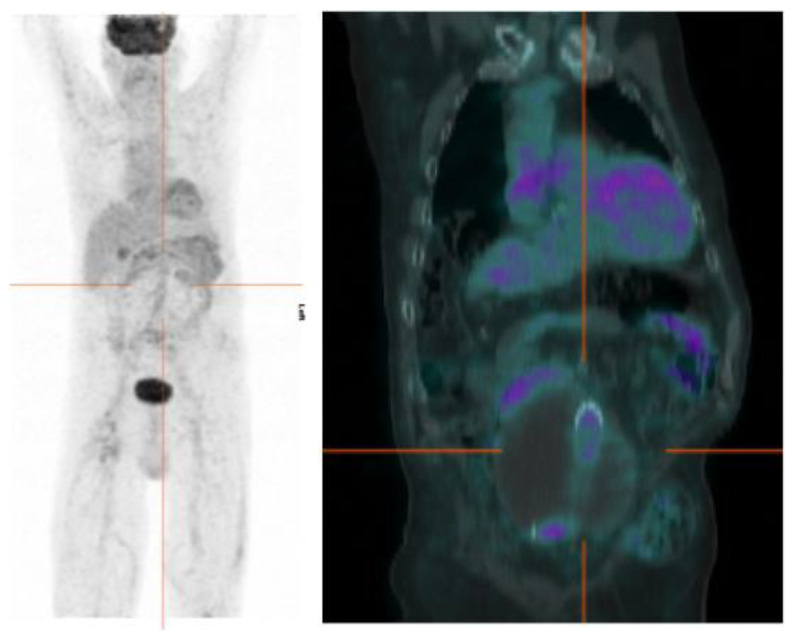
Vascular graft infection (VGI) is a rare but severe complication of vascular surgery that is associated with a bad prognosis and high mortality rate. An accurate and prompt identification of the infection and its extent is crucial for the correct management of the patient. However, standardized diagnostic algorithms and a univocal consensus on the best strategy to reach a diagnosis still do not exist. This review aims to summarize different radiological and Nuclear Medicine (NM) modalities commonly adopted for the imaging of VGI. Moreover, we attempt to provide evidence-based answers to several practical questions raised by clinicians and surgeons when they approach imaging in order to plan the most appropriate radiological or NM examination for their patients.
Keywords: FDG-PET/CT; WBC scintigraphy; angio-CT; infection; multimodality imaging; personalized medicine; vascular graft.
Conflict of interest statement
The authors declare no conflict of interest.
Figures
References
-
- Wilson W.R., Bower T.C., Creager M.A., Amin-Hanjani S., O’Gara P.T., Lockhart P.B., Darouiche R.O., Ramlawi B., Derdeyn C.P., Bolger A.F., et al. Vascular Graft Infections, Mycotic Aneurysms, and Endovascular Infections: A Scientific Statement from the American Heart Association. Circulation. 2016;134:e412–e460. doi: 10.1161/CIR.0000000000000457. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
