

Inconsistent descriptions of lumbar multifidus morphology: A scoping review
- PMID: 32429944
- PMCID: PMC7236939
- DOI: 10.1186/s12891-020-03257-7
Inconsistent descriptions of lumbar multifidus morphology: A scoping review
Abstract
Background: Lumbar multifidus (LM) is regarded as the major stabilizing muscle of the spine. The effects of exercise therapy in low back pain (LBP) are attributed to this muscle. A current literature review is warranted, however, given the complexity of LM morphology and the inconsistency of anatomical descriptions in the literature.
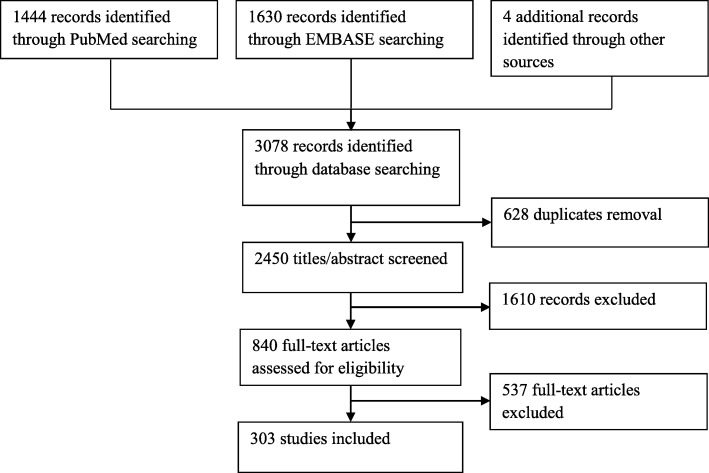
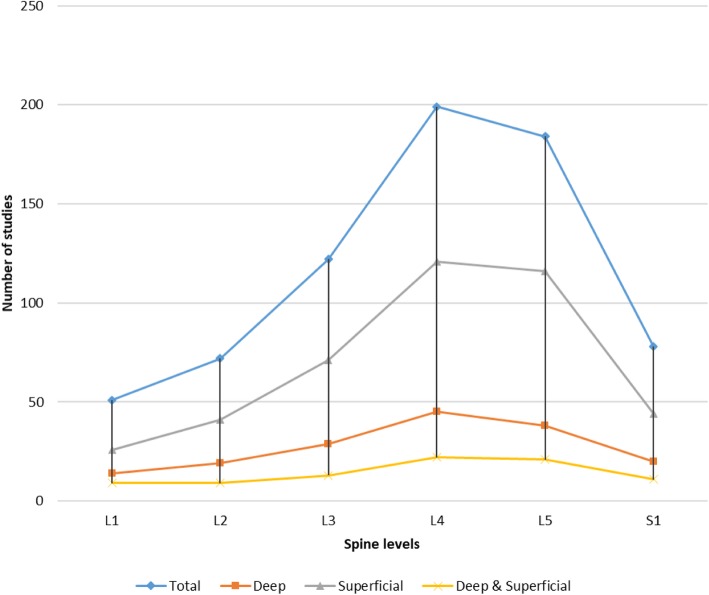
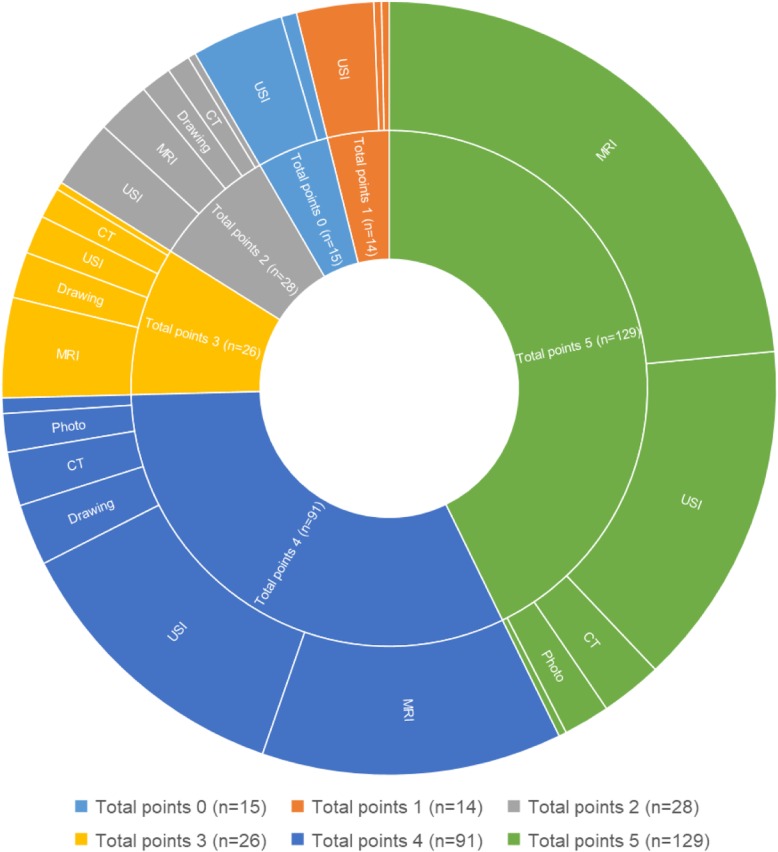
Methods: Scoping review of studies on LM morphology including major anatomy atlases. All relevant studies were searched in PubMed (Medline) and EMBASE until June 2019. Anatomy atlases were retrieved from multiple university libraries and online. All studies and atlases were screened for the following LM parameters: location, imaging methods, spine levels, muscle trajectory, muscle thickness, cross-sectional area, and diameter. The quality of the studies and atlases was also assessed using a five-item evaluation system.
Results: In all, 303 studies and 19 anatomy atlases were included in this review. In most studies, LM morphology was determined by MRI, ultrasound imaging, or drawings - particularly for levels L4-S1. In 153 studies, LM is described as a superficial muscle only, in 72 studies as a deep muscle only, and in 35 studies as both superficial and deep. Anatomy atlases predominantly depict LM as a deep muscle covered by the erector spinae and thoracolumbar fascia. About 42% of the studies had high quality scores, with 39% having moderate scores and 19% having low scores. The quality of figures in anatomy atlases was ranked as high in one atlas, moderate in 15 atlases, and low in 3 atlases.
Discussion: Anatomical studies of LM exhibit inconsistent findings, describing its location as superficial (50%), deep (25%), or both (12%). This is in sharp contrast to anatomy atlases, which depict LM predominantly as deep muscle. Within the limitations of the self-developed quality-assessment tool, high-quality scores were identified in a majority of studies (42%), but in only one anatomy atlas.
Conclusions: We identified a lack of standardization in the depiction and description of LM morphology. This could affect the precise understanding of its role in background and therapy in LBP patients. Standardization of research methodology on LM morphology is recommended. Anatomy atlases should be updated on LM morphology.
Keywords: Computer Tomography; Erector spinae; Lumbar Vertebrae; Lumbar multifidus; Magnetic Resonance Imaging; Paraspinal Muscles; Scoping review; Ultrasonography; low back pain.
Conflict of interest statement
The authors declare that they have no competing interests.
Figures
References
-
- Bagheri R, Takamjani IE, Dadgoo M, Sarrafzadeh J, Ahmadi A, Pourahmadi MR, et al. A protocol for clinical trial study of the effect of core stabilization exercises on spine kinematics during gait with and without load in patients with non-specific chronic low back pain. Chiropr Man Ther. 2017;25:31. - PMC - PubMed
-
- Sung PS, Yoon B, Lee DC. Lumbar spine stability for subjects with and without low back pain during one-leg standing test. Spine. 2010;35(16):E753–E760. - PubMed
-
- Wirth K, Hartmann H, Mickel C, Szilvas E, Keiner M, Sander A. Core stability in athletes: a critical analysis of current guidelines. Sports Med. 2017;47(3):401–414. - PubMed
-
- Hicks GE, Fritz JM, Delitto A, McGill SM. Preliminary development of a clinical prediction rule for determining which patients with low back pain will respond to a stabilization exercise program. Arch Phys Med Rehabil. 2005;86(9):1753–1762. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Miscellaneous
