

Outcomes in Patients With Hyperglycemia Affected by COVID-19: Can We Do More on Glycemic Control?
- PMID: 32430456
- PMCID: PMC7305003
- DOI: 10.2337/dc20-0723
Outcomes in Patients With Hyperglycemia Affected by COVID-19: Can We Do More on Glycemic Control?
Abstract
Objective: An important prognostic factor in any form of infection seems to be glucose control in patients with type 2 diabetes. There is no information about the effects of tight glycemic control on coronavirus disease 2019 (COVID-19) outcomes in patients with hyperglycemia. Therefore, we examined the effects of optimal glycemic control in patients with hyperglycemia affected by COVID-19.
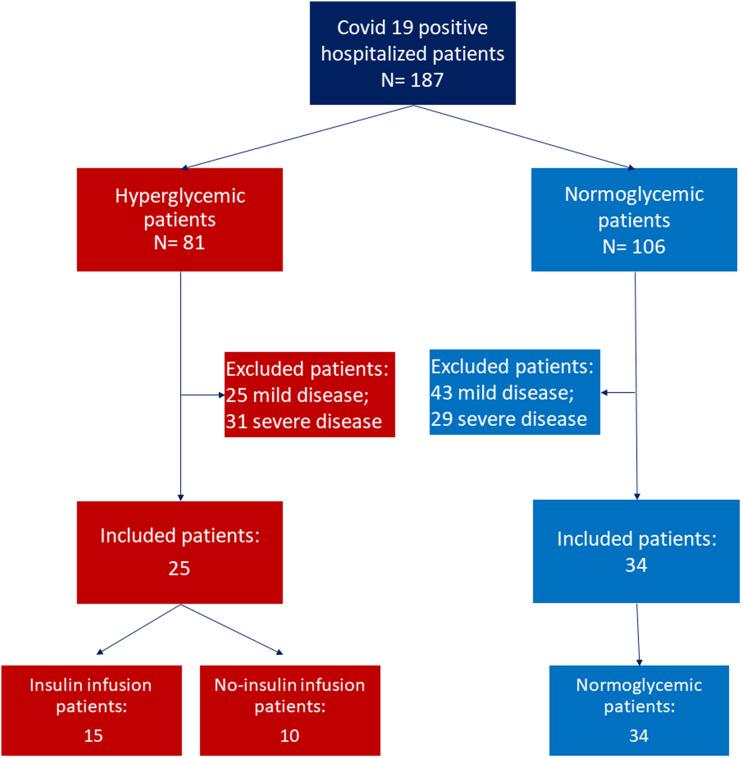
Research design and methods: Fifty-nine patients with COVID-19 hospitalized with moderate disease were evaluated. On the basis of admission glycemia >7.77 mmol/L, patients were divided into hyperglycemic and normoglycemic groups. Interleukin 6 (IL-6) and D-dimer levels were evaluated at admission and weekly during hospitalization. The composite end point was severe disease, admission to an intensive care unit, use of mechanical ventilation, or death.
Results: Thirty-four (57.6%) patients were normoglycemic and 25 (42.4%) were hyperglycemic. In the hyperglycemic group, 7 (28%) and 18 (72%) patients were diagnosed with diabetes already before admission, and 10 (40%) and 15 (60%) were treated without and with insulin infusion, respectively. The mean of glycemia during hospitalization was 10.65 ± 0.84 mmol/L in the no insulin infusion group and 7.69 ± 1.85 mmol/L in the insulin infusion group. At baseline, IL-6 and D-dimer levels were significantly higher in the hyperglycemic group than in the normoglycemic group (P < 0.001). Even though all patients were on standard treatment for COVID-19 infection, IL-6 and D-dimer levels persisted higher in patients with hyperglycemia during hospitalization. In a risk-adjusted Cox regression analysis, both patients with hyperglycemia and patients with diabetes had a higher risk of severe disease than those without diabetes and with normoglycemia. Cox regression analysis evidenced that patients with hyperglycemia treated with insulin infusion had a lower risk of severe disease than patients without insulin infusion.
Conclusions: Insulin infusion may be an effective method for achieving glycemic targets and improving outcomes in patients with COVID-19.
© 2020 by the American Diabetes Association.
Figures


References
-
- van Vught LA, Wiewel MA, Klein Klouwenberg PM, et al. Admission hyperglycemia in critically ill sepsis patients: association with outcome and host response. Crit Care Med 2016;44:1338–1346 - PubMed
-
- Thompson BT. Glucose control in sepsis. Clin Chest Med 2008;29:713–720, x - PubMed
-
- Tiwari S, Pratyush DD, Gahlot A, Singh SK. Sepsis in diabetes: a bad duo. Diabetes Metab Syndr 2011;5:222–227 - PubMed
-
- Esposito K, Nappo F, Marfella R, et al. Inflammatory cytokine concentrations are acutely increased by hyperglycemia in humans: role of oxidative stress. Circulation 2002;106:2067–2072 - PubMed
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Medical
Molecular Biology Databases
