

Cross-Resistance Among Next-Generation Antiandrogen Drugs Through the AKR1C3/AR-V7 Axis in Advanced Prostate Cancer
- PMID: 32430485
- PMCID: PMC8855880
- DOI: 10.1158/1535-7163.MCT-20-0015
Cross-Resistance Among Next-Generation Antiandrogen Drugs Through the AKR1C3/AR-V7 Axis in Advanced Prostate Cancer
Abstract
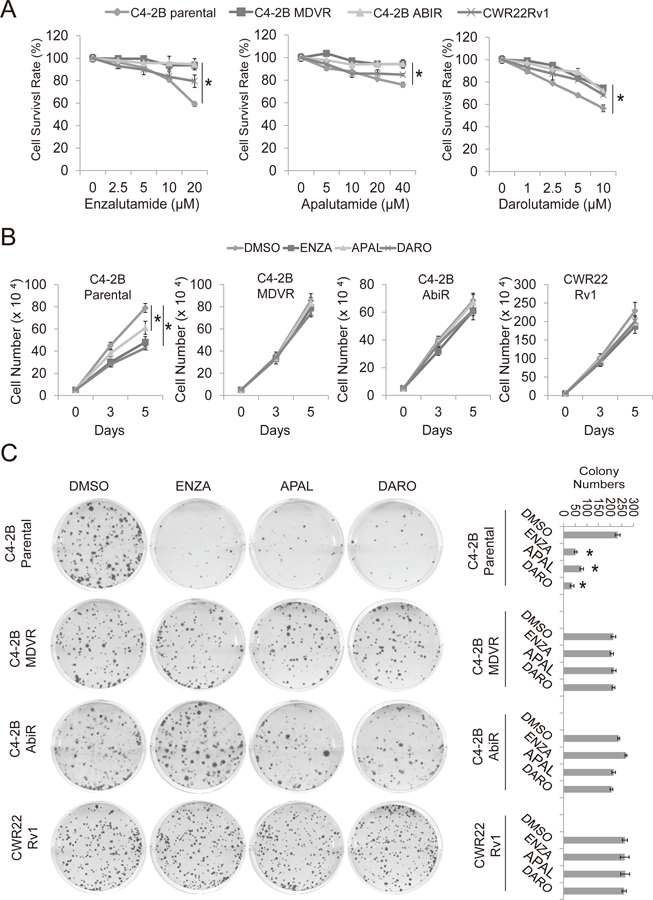
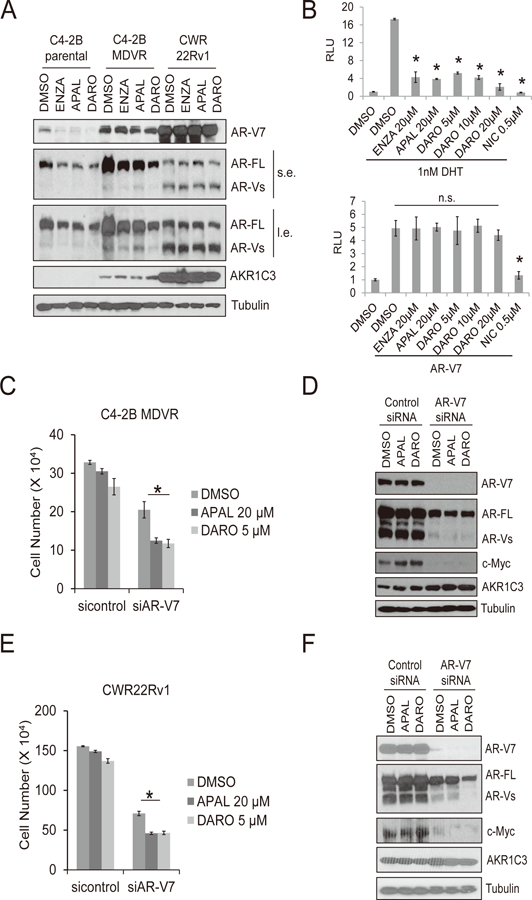
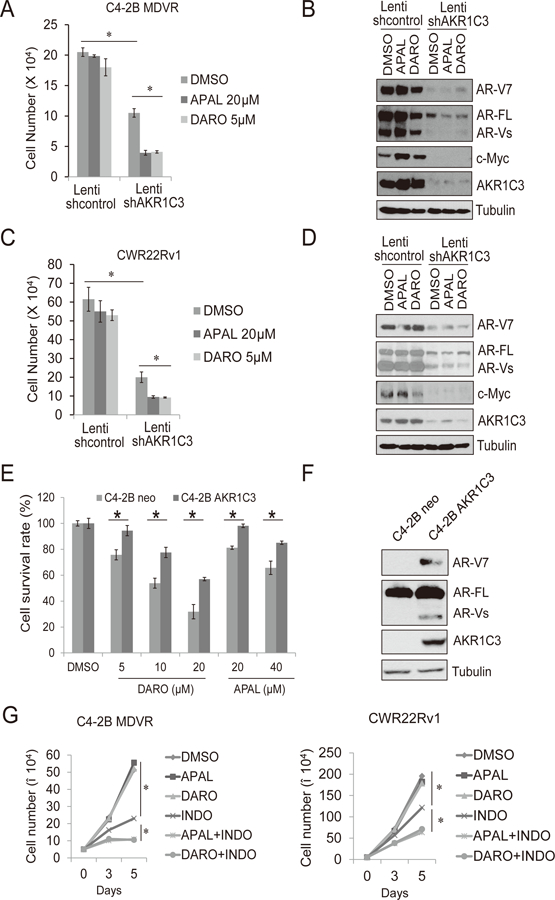
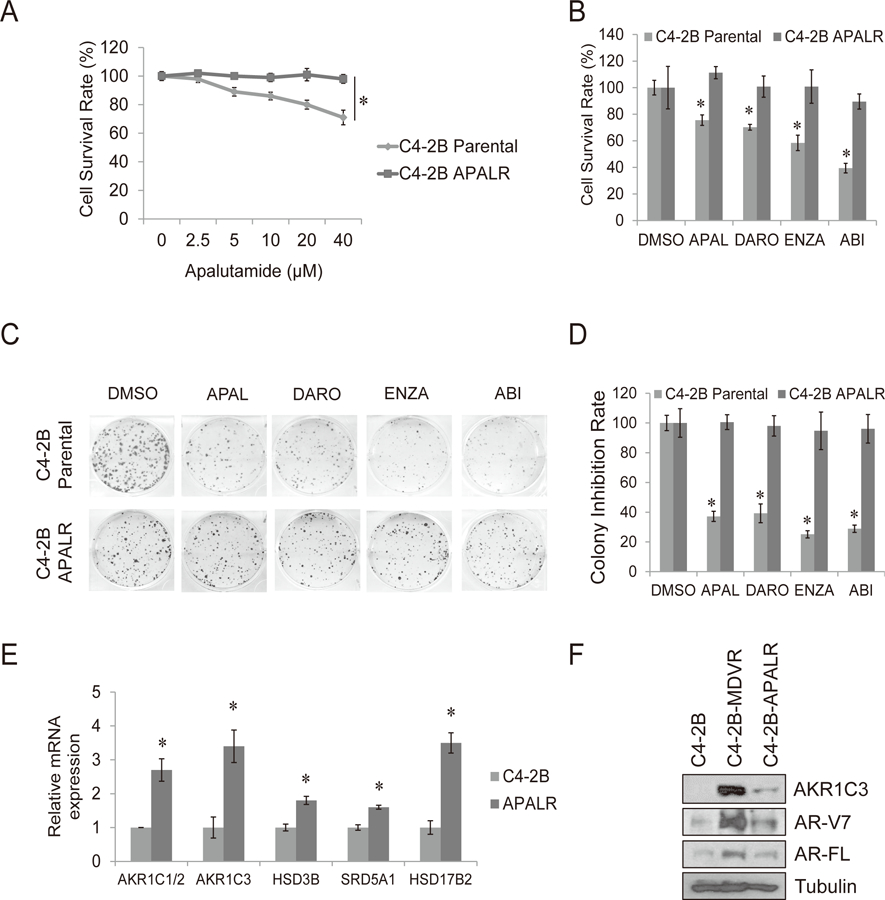
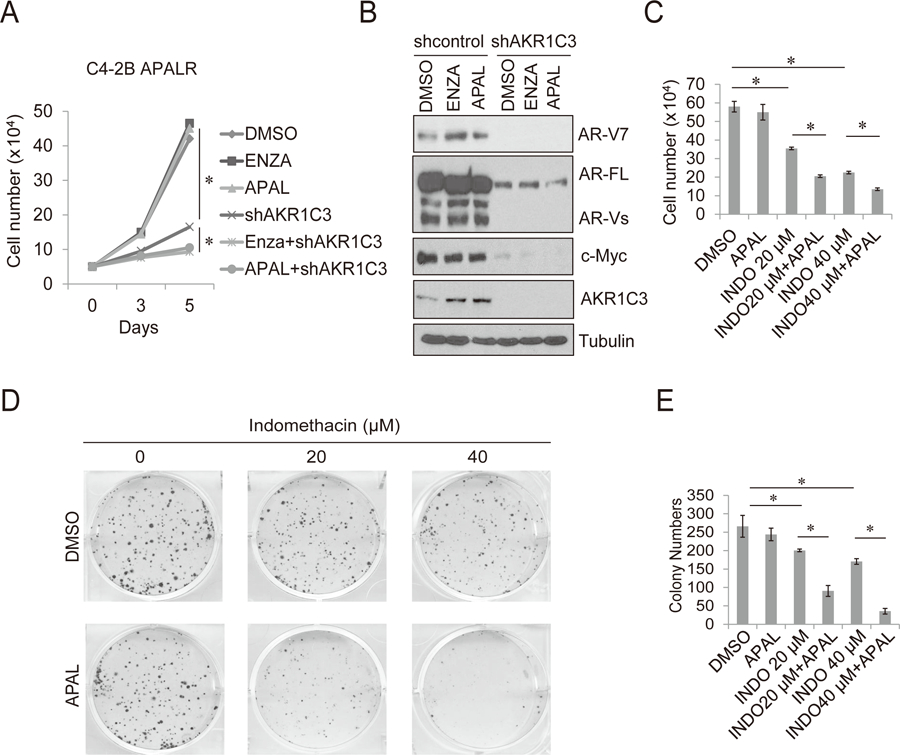
The next-generation antiandrogen drugs, XTANDI (enzalutamide), ZYTIGA (abiraterone acetate), ERLEADA (apalutamide) and NUBEQA (darolutamide) extend survival times and improve quality of life in patients with advanced prostate cancer. Despite these advances, resistance occurs frequently and there is currently no definitive cure for castration-resistant prostate cancer. Our previous studies identified that similar mechanisms of resistance to enzalutamide or abiraterone occur following treatment and cross-resistance exists between these therapies in advanced prostate cancer. Here, we show that enzalutamide- and abiraterone-resistant prostate cancer cells are further cross-resistant to apalutamide and darolutamide. Mechanistically, we have determined that the AKR1C3/AR-V7 axis confers this cross-resistance. Knockdown of AR-V7 in enzalutamide-resistant cells resensitize cells to apalutamide and darolutamide treatment. Furthermore, targeting AKR1C3 resensitizes resistant cells to apalutamide and darolutamide treatment through AR-V7 inhibition. Chronic apalutamide treatment in C4-2B cells activates the steroid hormone biosynthesis pathway and increases AKR1C3 expression, which confers resistance to enzalutamide, abiraterone, and darolutamide. In conclusion, our results suggest that apalutamide and darolutamide share similar resistant mechanisms with enzalutamide and abiraterone. The AKR1C3/AR-V7 complex confers cross-resistance to second-generation androgen receptor-targeted therapies in advanced prostate cancer.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures
References
-
- Holzbeierlein J, Lal P, LaTulippe E, Smith A, Satagopan J, Zhang L, et al. Gene expression analysis of human prostate carcinoma during hormonal therapy identifies androgen-responsive genes and mechanisms of therapy resistance. The American journal of pathology 2004;164(1):217–27 doi 10.1016/S0002-9440(10)63112-4. - DOI - PMC - PubMed
-
- Scher HI, Sawyers CL. Biology of progressive, castration-resistant prostate cancer: directed therapies targeting the androgen-receptor signaling axis. Journal of clinical oncology : official journal of the American Society of Clinical Oncology 2005;23(32):8253–61 doi 10.1200/JCO.2005.03.4777. - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
