

Evaluation of the bronchial arteries: normal findings, hypertrophy and embolization in patients with hemoptysis
- PMID: 32430593
- PMCID: PMC7237606
- DOI: 10.1186/s13244-020-00877-4
Evaluation of the bronchial arteries: normal findings, hypertrophy and embolization in patients with hemoptysis
Abstract
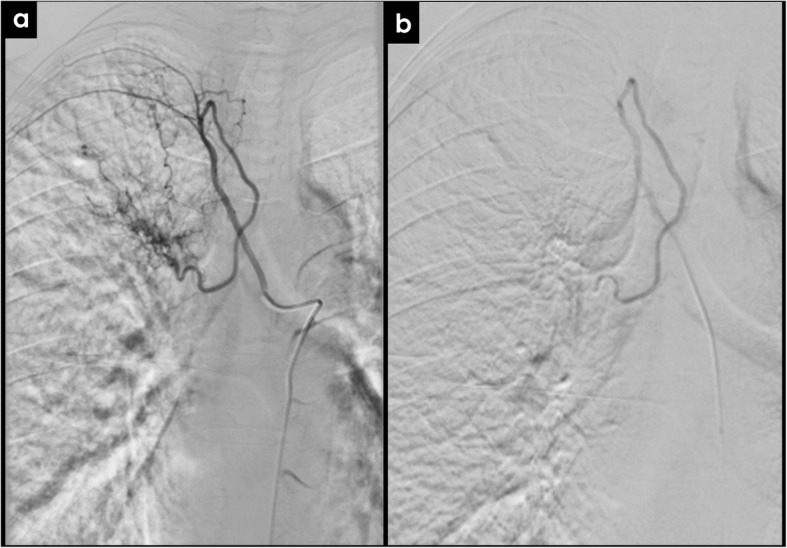
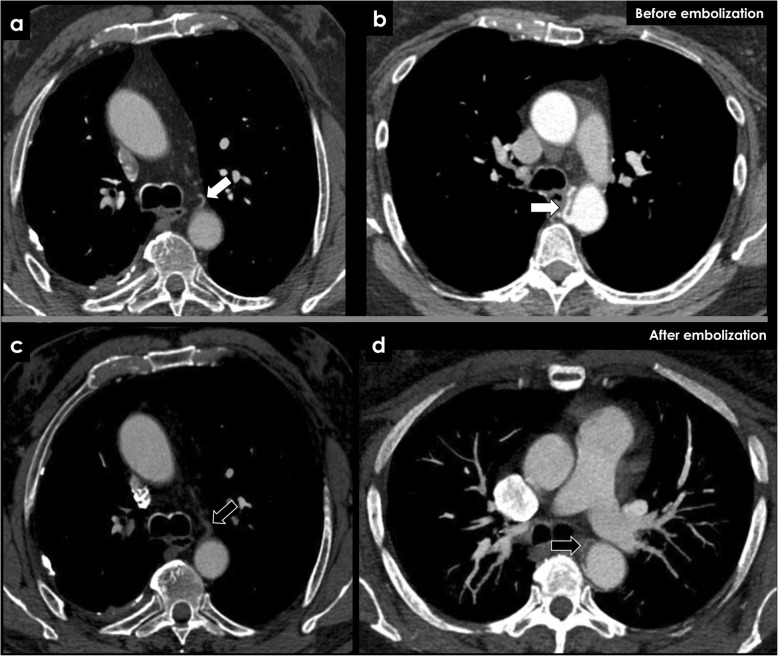
The enlargement of the bronchial arteries occurs in a multitude of congenital and acquired diseases and is responsible for the majority of cases of hemoptysis. In this review, we provide a simplified imaging approach to the evaluation of the bronchial arteries. We highlight the anatomy and function of the bronchial arteries, typical imaging findings, how to recognize bronchial artery dilatation, and its underlying causes. Contrast-enhanced computer tomography plays a major role in diagnosing bronchial artery enlargement and also improves treatment planning. Bronchial artery embolization has proven to be effective in controlling the potential hazardous hemoptysis.
Keywords: Angiography; Bronchial arteries; Computer tomography; Embolization; Hemoptysis.
Conflict of interest statement
The authors declare that they have no competing interests
Figures




References
-
- Bruzzi John F., Rémy-Jardin Martine, Delhaye Damien, Teisseire Antoine, Khalil Chadi, Rémy Jacques. Multi–Detector Row CT of Hemoptysis. RadioGraphics. 2006;26(1):3–22. - PubMed
-
- Pump KK. Distribution of bronchial arteries in the human lung. Chest. 1972;62:447–451. - PubMed
-
- Jean-Baptiste E. Clinical assessment and management of massive hemoptysis. Crit Care Med. 2000;28:1642–1647. - PubMed
-
- Tanomkiat W, Tanisaro K. Radiographic relationship of the origin of the bronchial arteries to the left main bronchus. J Thorac Imaging. 2003;18:27–33. - PubMed
-
- Hartmann Ieneke J. C., Remy-Jardin Martine, Menchini Laura, Teisseire Antoine, Khalil Chadi, Remy Jacques. Ectopic origin of bronchial arteries: assessment with multidetector helical CT angiography. European Radiology. 2007;17(8):1943–1953. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
