

Clinical applications of digital angiography with the harmonization function in body interventional radiology
- PMID: 32430663
- PMCID: PMC7529630
- DOI: 10.1007/s11604-020-00990-w
Clinical applications of digital angiography with the harmonization function in body interventional radiology
Abstract
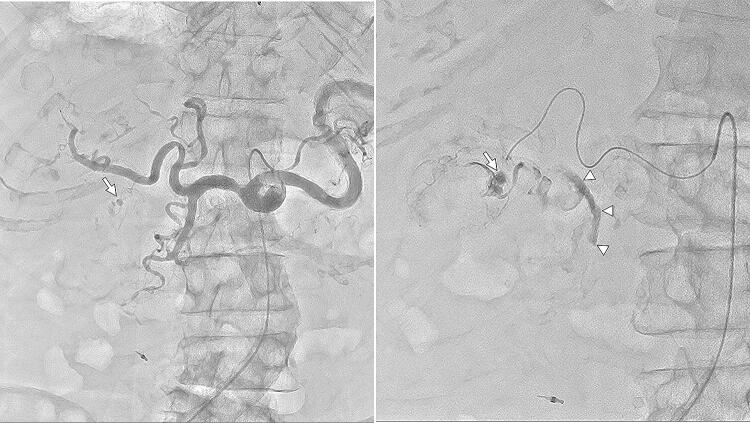
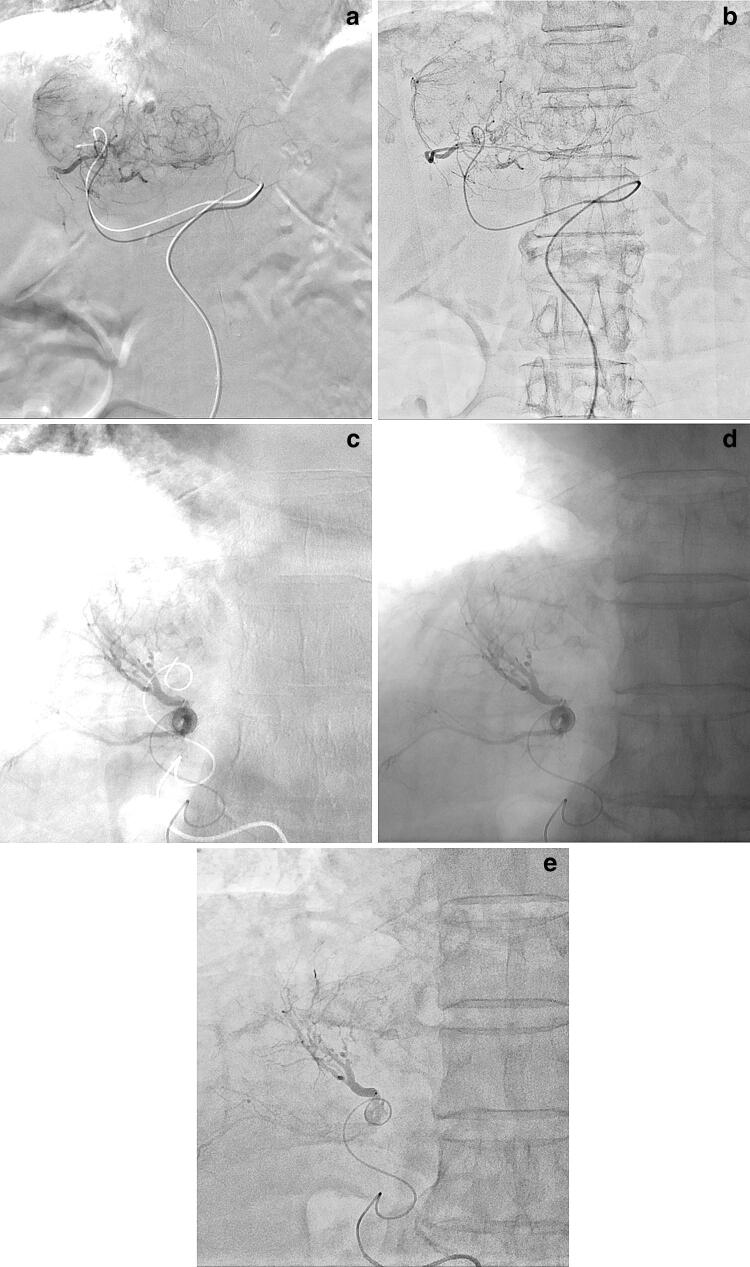
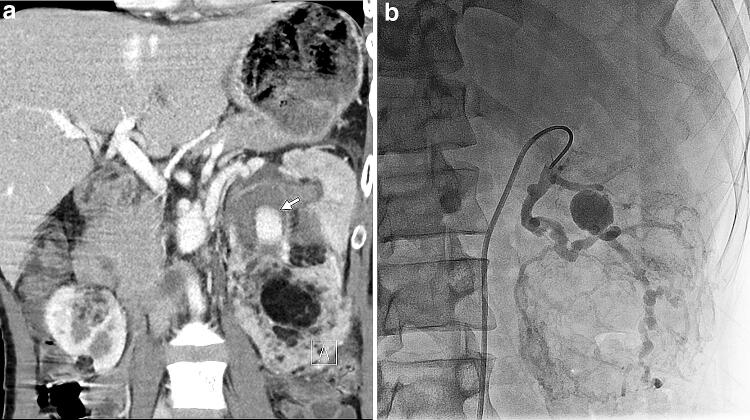
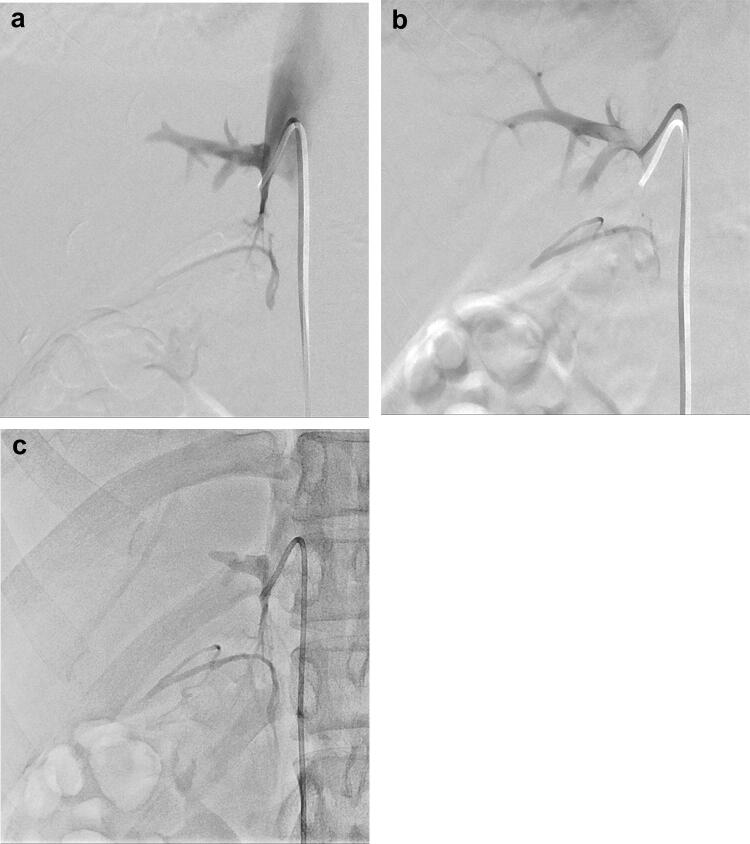
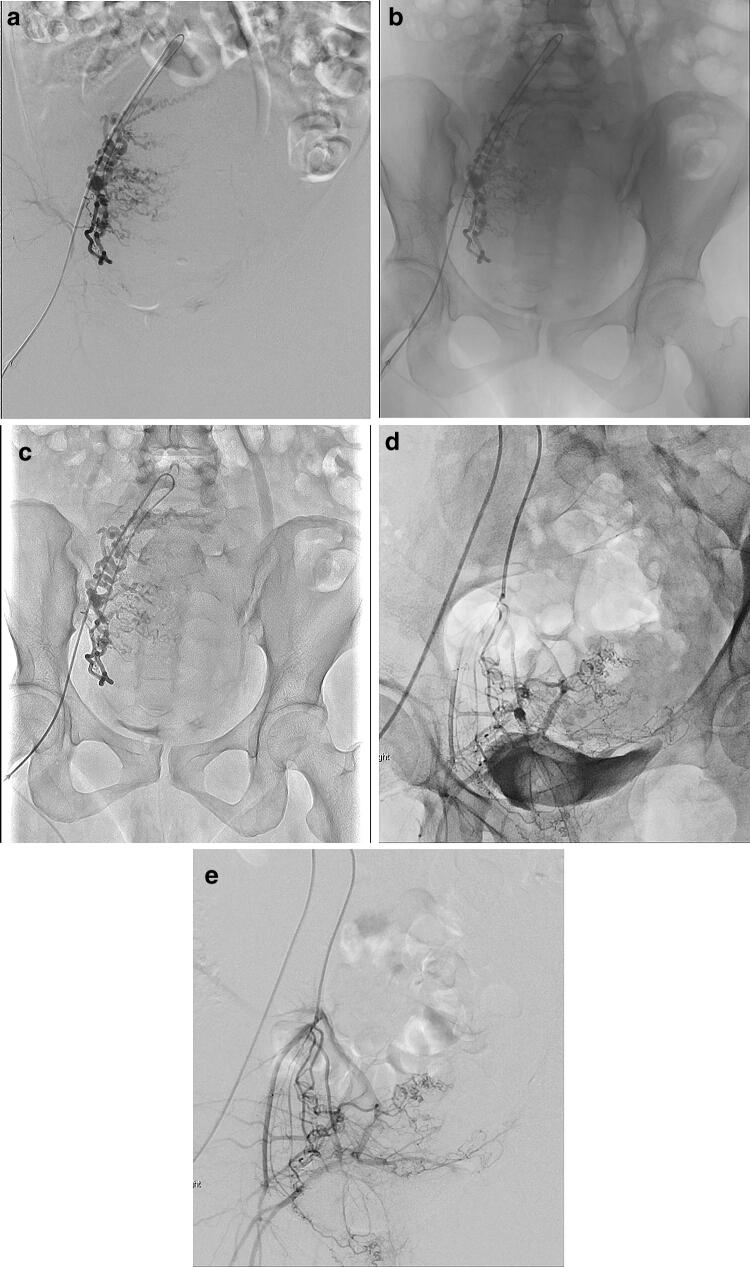
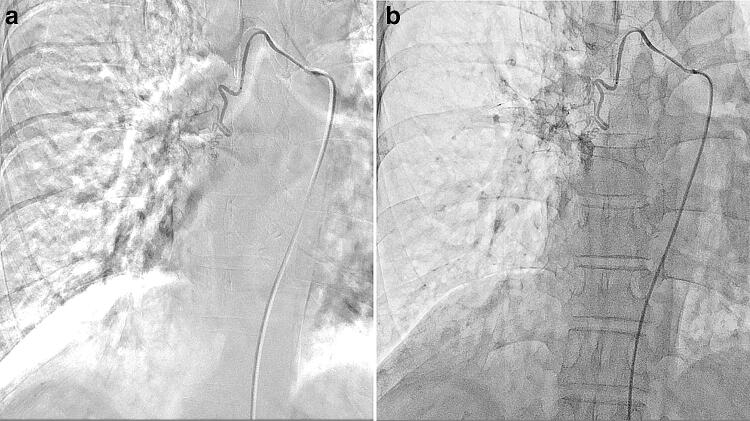
Digital subtraction angiography (DSA) is frequently applied in interventional radiology (IR). When DSA is not useful due to misregistration, digital angiography (DA) as an alternative option is used. In DA, the harmonization function (HF) works in real time by harmonizing the distribution of gray steps or reducing the dynamic range; thus, it can compress image gradations, decrease image contrast, and suppress halation artifacts. DA with HF as a good alternative to DSA is clinically advantageous in body IR for generating DSA-like images and simultaneously reducing various motion artifacts and misregistrations caused by patient body motion, poor breath-holding, bowel and ureter peristalsis, and cardiac pulsation as well as halation artifacts often stemming from the lung field. Free-breath DA with HF can improve body IR workflow and decrease the procedure time by reducing the risk of catheter dislocation and using background structures as anatomical landmarks, demonstrating reduced radiation exposure relative to DSA. Thus, HF should be more widely and effectively utilized for appropriate purposes in body IR. This article illustrates the basic facts and principles of HF in DA, and demonstrates clinical advantages and limitations of this function in body IR.
Keywords: Digital angiography; Dynamic density optimization; Harmonization function; Interventional radiology; Radiation exposure.
Figures
References
-
- Brody WR. Digital subtraction angiography. IEEE Trans Nucl Sci. 1982;29:1176–1180. doi: 10.1109/TNS.1982.4336336. - DOI
-
- Meijering EHW, Zuiderveld KJ, Viergever MA. Image registration for digital subtraction angiography. Int J Comput Vis. 1999;31:227–246. doi: 10.1023/A:1008074100927. - DOI
-
- Skau T, Bolin T, Karner G. Digital subtraction angiography versus standard contrast arteriography in evaluation of peripheral vascular disease. Int Angiol. 1988;7:42–45. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Research Materials
Miscellaneous
