

Adenocarcinoma of the lung: from BAC to the future
- PMID: 32430670
- PMCID: PMC7237554
- DOI: 10.1186/s13244-020-00875-6
Adenocarcinoma of the lung: from BAC to the future
Abstract
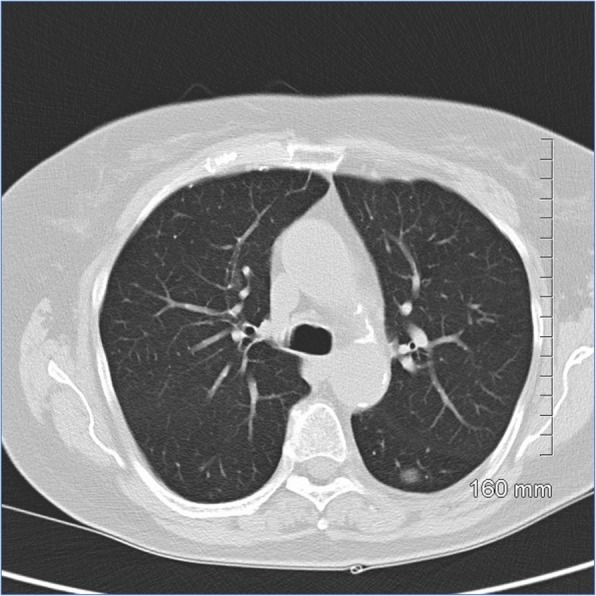
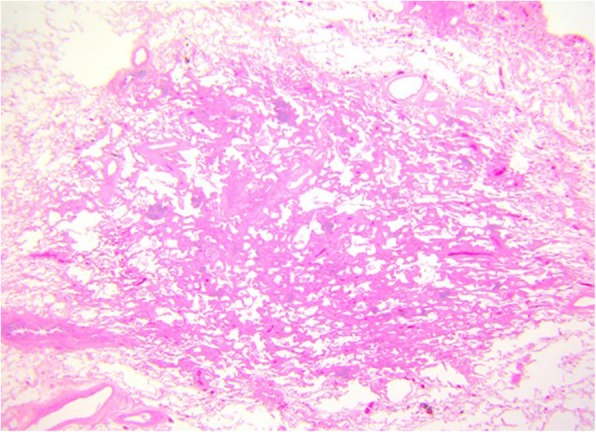
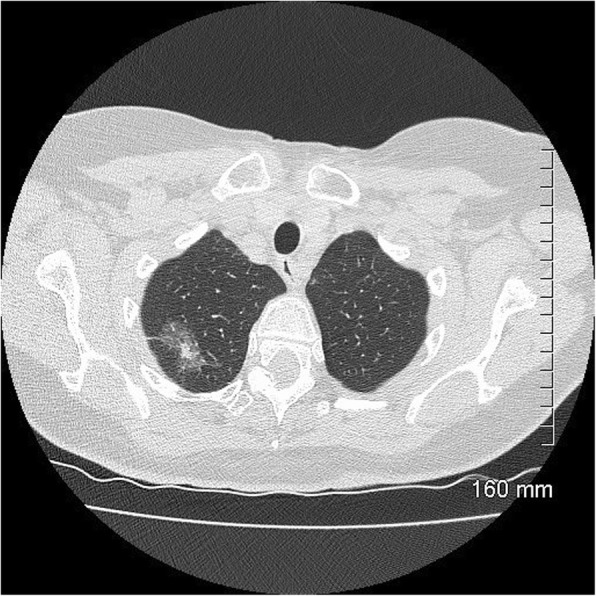
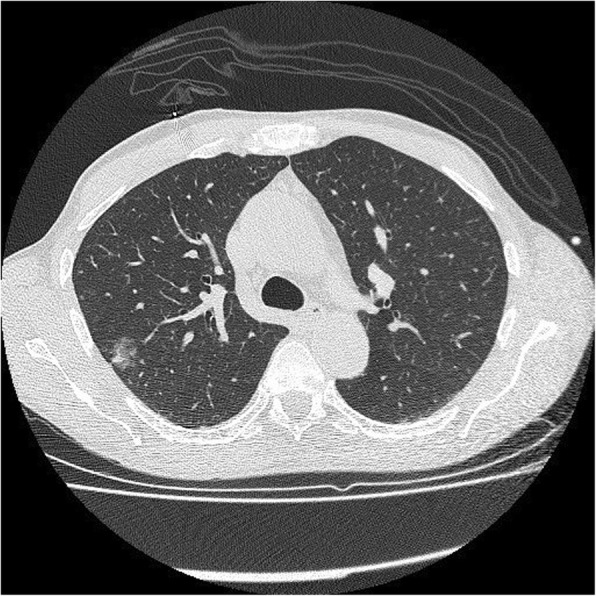
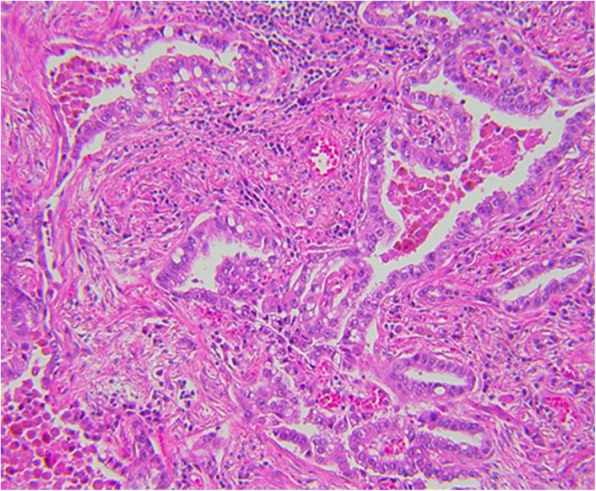
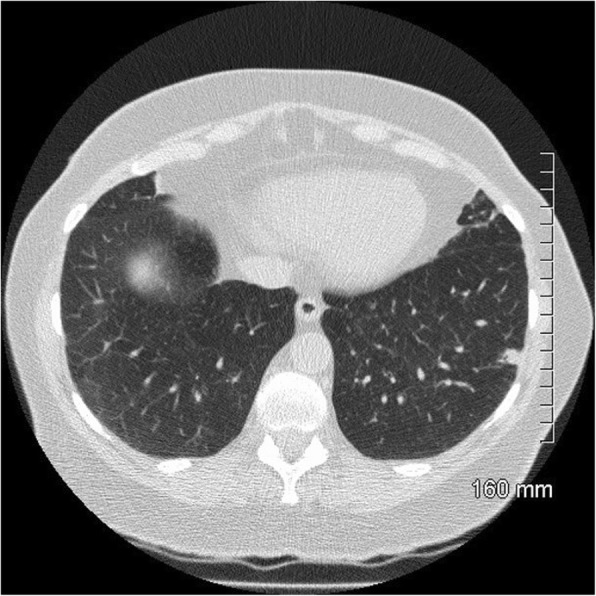
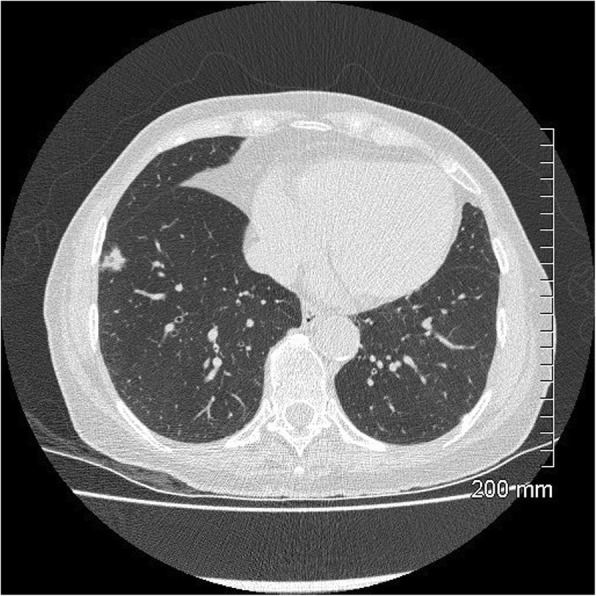
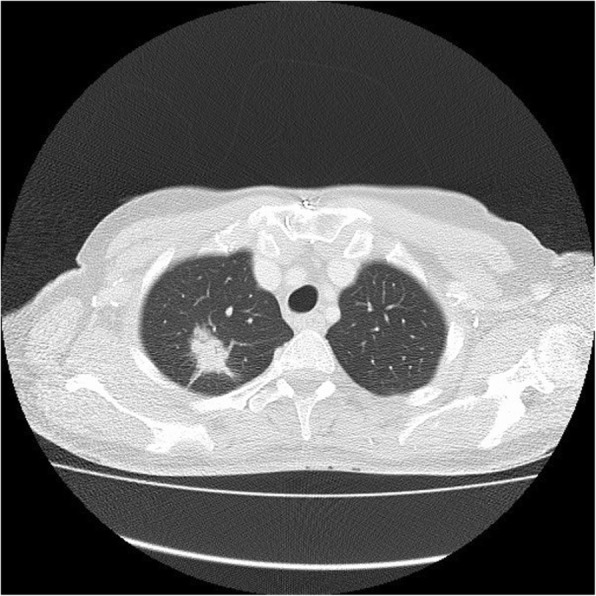
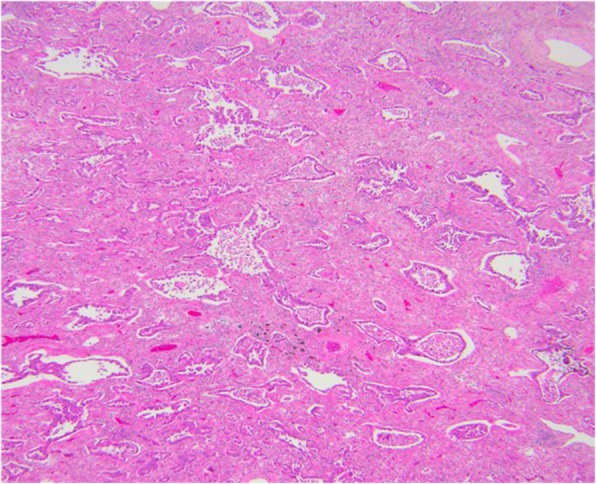
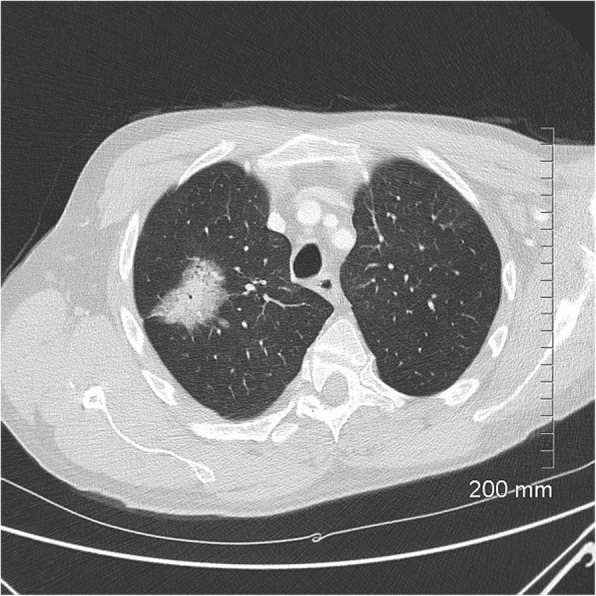
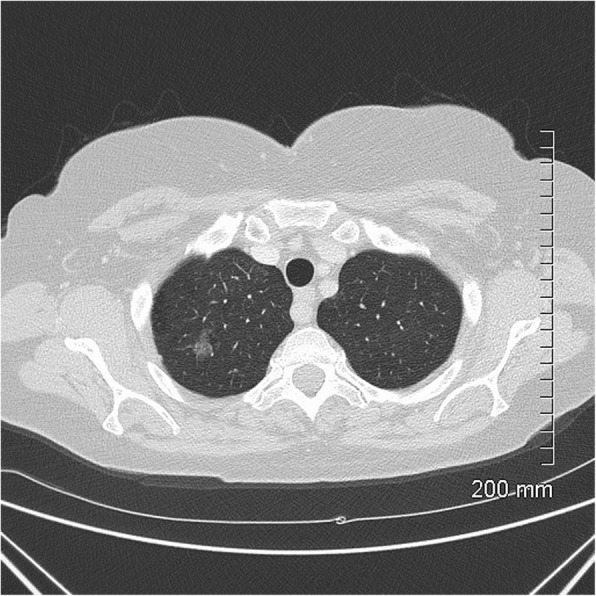
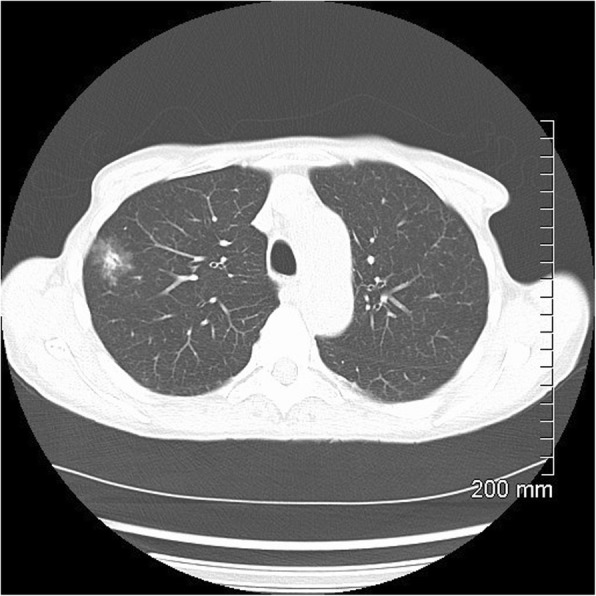
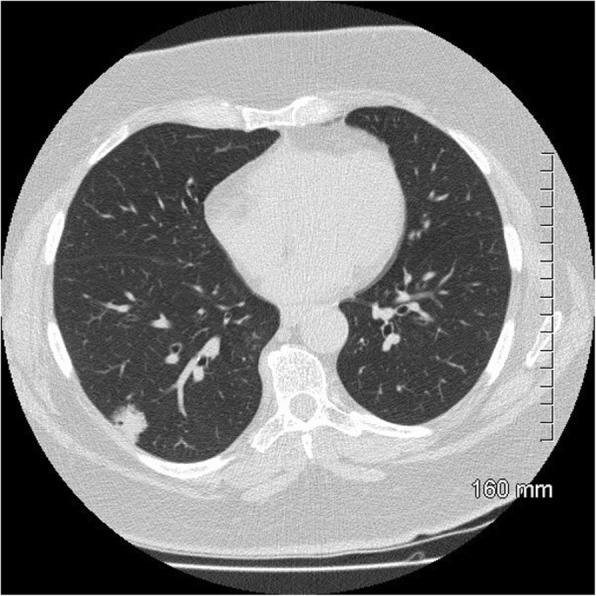
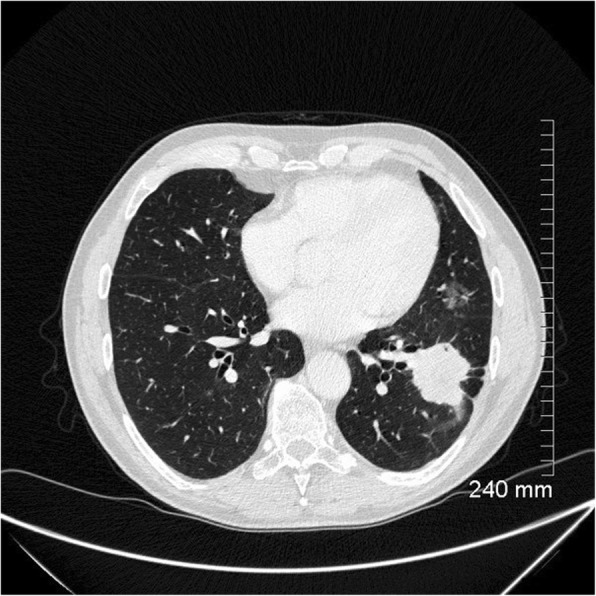
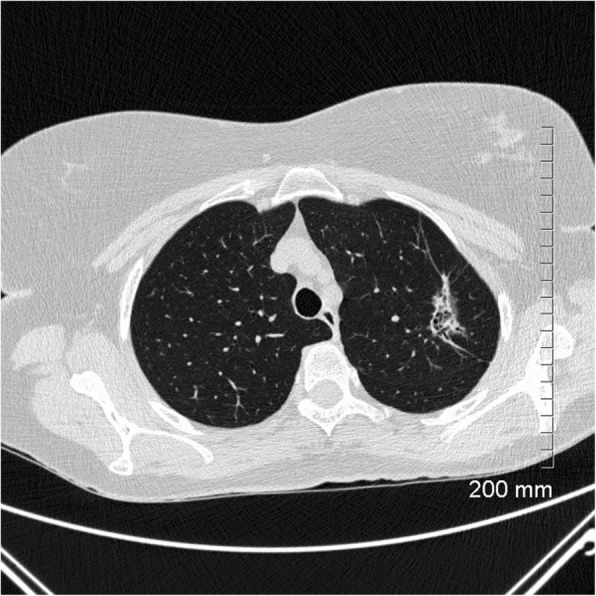
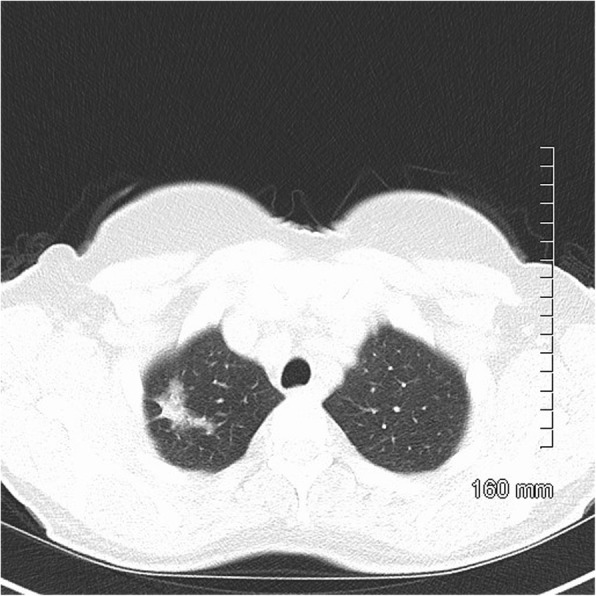
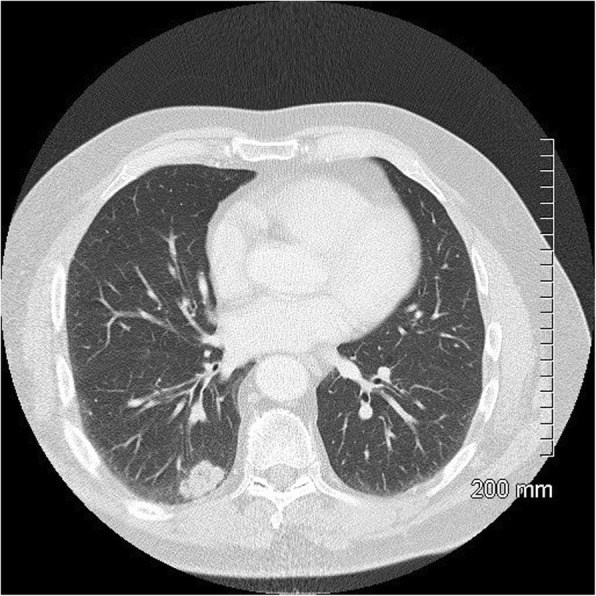
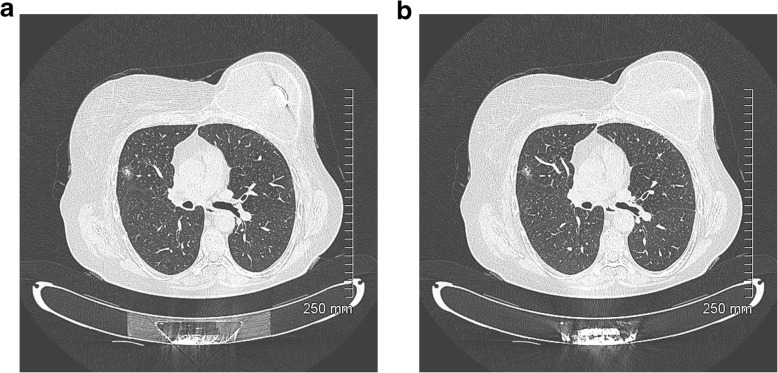
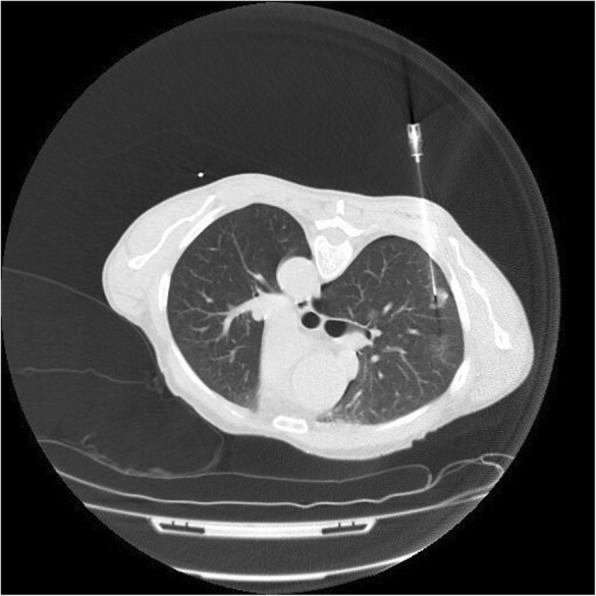
Adenocarcinoma in situ, minimally invasive adenocarcinoma, lepidic predominant adenocarcinoma and invasive mucinous adenocarcinoma are relatively new classification entities which replace the now retired term, bronchoalveolar carcinoma (BAC). The radiographic appearance of these lesions ranges from pure, ground glass nodules to large, solid masses. A thorough understanding of the new classification is essential to radiologists who work with MDT colleagues to provide accurate staging and treatment. A 2-year review was performed of all surgically resected cases of adenocarcinoma in situ, minimally invasive adenocarcinoma and lepidic predominant adenocarcinoma in our institution. Cases are broken down by age, gender, tumour type and tumour location. A pictorial review is presented to illustrate the radiologic and pathologic features of each entity.
Keywords: Computed tomography; Lung adenocarcinoma; Pathology; Solitary pulmonary nodule; Subsolid nodules.
Conflict of interest statement
Not applicable
Figures
References
-
- Travis WD, Garg K, Franklin WA, et al. Evolving concepts in the pathology and computed tomography imaging of lung adenocarcinoma and bronchioloalveolar carcinoma. J Clin Oncol. 2005;23(14):3279–3287. - PubMed
-
- Travis WD, Travis LB, Devesa SS. Lung cancer. Cancer. 1995;75(1 Suppl):191–202. - PubMed
-
- Malassez L (1876) Examen histologique d’un cas de cancer encephaloide du poumon (epithelioma). Arch Physiol Norm Pathol 1876;3:353-72 [Google Scholar].
-
- Musser JH (1903) Primary cancer of the lung. U Penn Med Bull 1903:16:289-96 [Google Scholar].
-
- Sweany HC (1935) A so-called alveolar cell cancer of the lung. Arch Pathol 1935;19:203-7 [Google Scholar].
Publication types
LinkOut - more resources
Full Text Sources
