

Spectrum of imaging findings in AIDS-related diffuse large B cell lymphoma
- PMID: 32430699
- PMCID: PMC7237590
- DOI: 10.1186/s13244-020-00871-w
Spectrum of imaging findings in AIDS-related diffuse large B cell lymphoma
Abstract
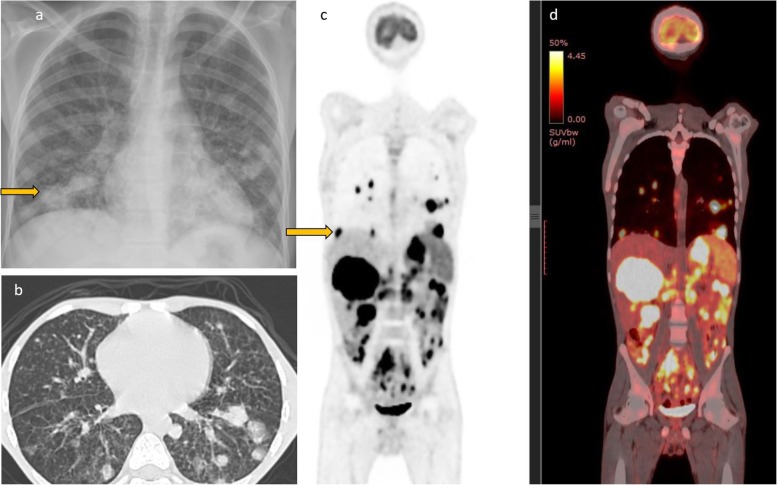
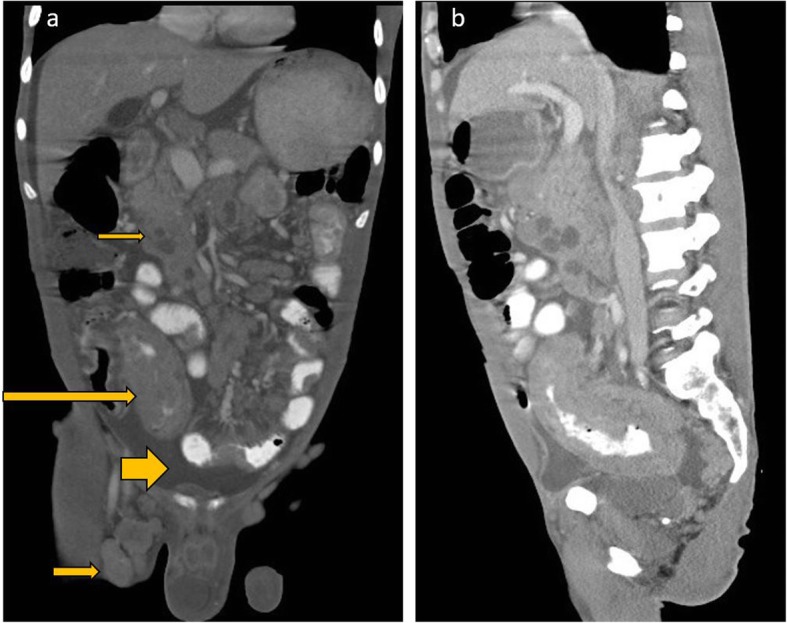
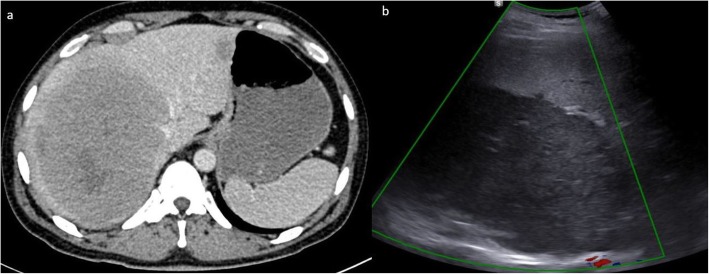
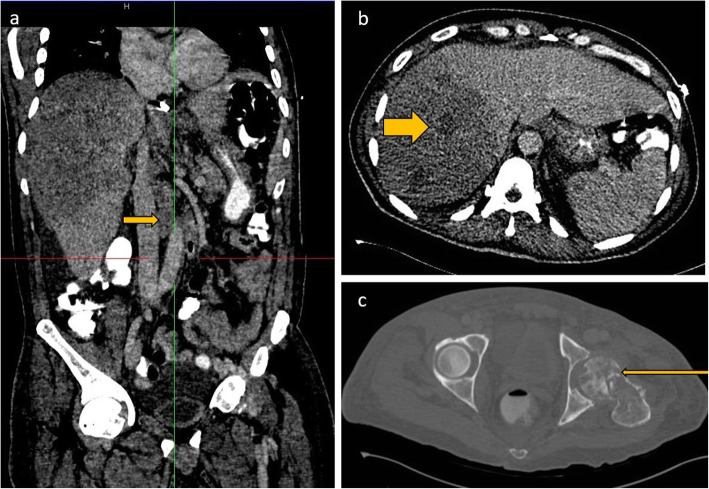
Lymphoma in HIV-infected patients is AIDS defining. This is the second most common AIDS defining malignancy after Kaposi's sarcoma. Development of lymphoma in HIV patients is related to immunosuppression and high viral load. Co-infection with other lymphotrophic viruses especially EBV is also strongly associated with development of lymphoma in HIV patients. Despite advances in HAART therapy, incidence of diffuse large B cell lymphoma in HIV-infected patients remains significantly higher than in the general population.Early diagnosis is challenging due to presence of opportunistic infections and atypical presentation of the lymphoma in this subset of patients. Atypical imaging findings are not unusual, and the diagnosis of lymphoma on imaging is on many occasions unexpected as the patient would ideally be initially investigated for presumed opportunistic infection.Lymphoma treatment approaches in HIV patients are complicated by comorbidity with opportunistic infections and performance status of the patients. Treatment failure and early relapse are also common in AIDS-related lymphoma. This review article highlights the common and unusual multimodality imaging findings in HIV-associated lymphoma.
Keywords: AIDS-related diffuse large B cell lymphoma; Extranodal lymphoma; HIV and malignancy; Multimodality imaging of lymphoma.
Conflict of interest statement
No competing interests
Figures
References
-
- Global HIV & AIDS statistics — 2019 fact sheet. Available via: https://www.unaids.org/en/resources/fact-sheet.
-
- Kaplan LD, Ai W (2019) AIDS-related lymphomas: epidemiology, risk factors, and pathobiology. https://www.uptodate.com/contents/hiv-related-lymphomas-epidemiology-ris.... Accesed 14 Oct 2019.
-
- Javadi Sanaz, Menias Christine O., Karbasian Niloofar, Shaaban Akram, Shah Komal, Osman Adam, Jensen Corey T., Lubner Meghan G., Gaballah Ayman H., Elsayes Khaled M. HIV-related Malignancies and Mimics: Imaging Findings and Management. RadioGraphics. 2018;38(7):2051–2068. doi: 10.1148/rg.2018180149. - DOI - PubMed
Publication types
LinkOut - more resources
Full Text Sources
