

The role of contrast-enhanced ultrasound (CEUS) in the evaluation of scrotal trauma: a review
- PMID: 32430792
- PMCID: PMC7237587
- DOI: 10.1186/s13244-020-00874-7
The role of contrast-enhanced ultrasound (CEUS) in the evaluation of scrotal trauma: a review
Abstract
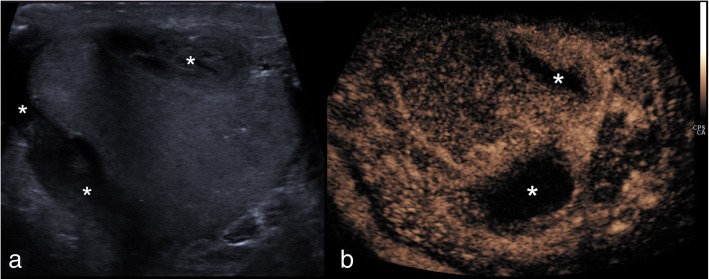
Testicular trauma is common, usually trivial and rarely requires hospital attendance, but if it does, then imaging becomes essential as scrotal assessment may be difficult due to pain and/or scrotal disruption. Ultrasound (US) assumes a crucial role as other cross-sectional modalities have a limited use in the acute presentation. Despite the acceptable accuracy of conventional US techniques, there are limitations which hinder a thorough evaluation, critically the assessment of tissue viability, crucial for clinical management and prognosis. Contrast-enhanced ultrasound (CEUS) has been shown to offer improved flow visualisation and tissue perfusion compared with conventional Doppler techniques. CEUS can accurately and confidently demonstrate the viability of testicular parenchyma, delineate fracture lines and haematomas and guide treatment for testis-sparing surgery or orchidectomy. The purpose of this review is to present the literature, familiarise physicians with the principles of CEUS and findings of scrotal trauma and illustrate the main abnormalities through characteristic and educative cases.
Keywords: Contrast-enhanced ultrasound; Haematoma; Scrotal trauma; Testicular trauma; Testis-sparing surgery.
Conflict of interest statement
PS has received lecture fees from Bracco, Siemens, Samsung, Philips and Hitachi. GTY has received lecture fees from Siemens and Bracco. MES has received lecture fees from Bracco. DYH has received lecture fees from Bracco. The rest of the authors have no conflict of interest regarding the publication of this manuscript.
Figures







References
-
- Sidhu Paul S. Clinical Ultrasound. 2011. Diseases of the testis and epididymis; pp. 593–620.
Publication types
LinkOut - more resources
Full Text Sources
