

Dissociation between Cervical Mucus and Urinary Hormones during the Postpartum Return of Fertility in Breastfeeding Women
- PMID: 32431376
- PMCID: PMC6322125
- DOI: 10.1177/0024363918809698
Dissociation between Cervical Mucus and Urinary Hormones during the Postpartum Return of Fertility in Breastfeeding Women
Abstract
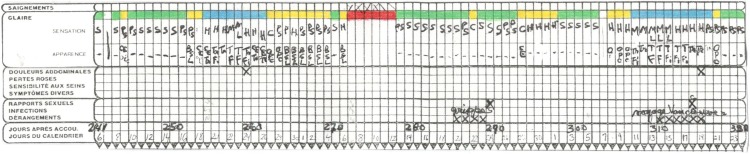
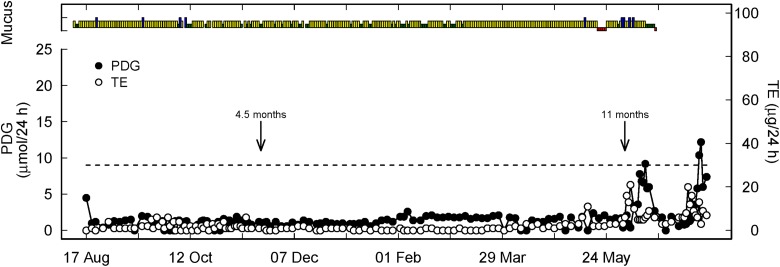
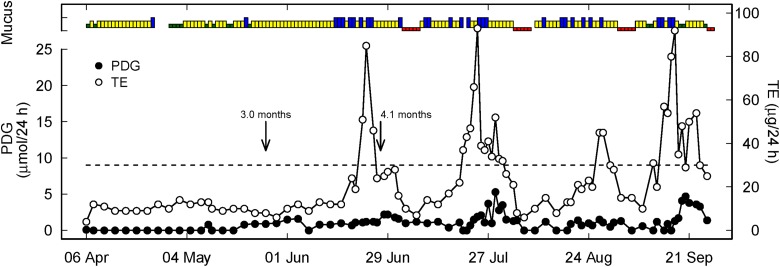
Identifying the return of fertility with cervical mucus observations is challenging during the postpartum period. Use of urinary measurements of estrogen and progesterone can assist in understanding the return to fertility during this period. The purposes of this study were to describe the postpartum return of fertility by an analysis of total estrogen (TE) and pregnanediol glucuronide (PDG) profiles and to correlate these profiles with cervical mucus observations. Twenty-six participants collected urine samples during the postpartum period and recorded mucus scores. TE and PDG hormones were analyzed and compared with mucus scores. During amenorrhea, mucus reflected TE changes in only 35 percent of women; after amenorrhea, typical mucus patterns were seen in 33 percent of cycles. We concluded that postpartum mucus and hormone profiles are significantly dissociated but that monitoring urinary hormones may assist in identifying the return of fertility. We also identified different hormonal patterns in the return to fertility. The postpartum period is a challenging time for identifying the return of fertility. The purposes of this study were to describe the hormonal patterns during the return of fertility and to correlate these patterns with cervical mucus observations. Twenty-six postpartum women collected urine samples and recorded mucus scores. Urinary estrogen and progesterone hormones were analyzed and compared with mucus scores. Before the return of menses, mucus reflected hormonal changes in only 35 percent women and after first menses in 33 percent of cycles. We found that hormone profiles do not correlate well with mucus observations during the postpartum return of fertility.
Keywords: Breastfeeding; Estrone-3-glucuronide; Natural family planning; Postpartum; Pregnanediol.
© Catholic Medical Association 2018.
Conflict of interest statement
Declaration of Conflicting Interests: The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Figures
References
-
- Academy of Breastfeeding Medicine Protocol Committee. 2006. ABM clinical protocol# 13: contraception during breastfeeding. Breastfeeding Medicine 1(1): 43–51. - PubMed
-
- Arevalo M., Jennings V., Sinai I. 2003. “Application of Simple Fertility Awareness-based Methods of Family Planning to Breastfeeding Women.” Fertility and Sterility 80:1241–48. - PubMed
-
- Bigelow J. L., Dunson D. B., Stanford J. B., Ecochard R., Gnoth C., Colombo B. 2004. “Mucus Observations in the Fertile Window: A Better Predictor of Conception than Timing of Intercourse.” Human Reproduction 19:889–92. doi: 10.1093/humrep/deh173. - PubMed
-
- Blackwell L. F., Brown J. B., Vigil P., Gross B., Sufi S., d’Arcangues C. 2003. “Hormonal Monitoring of Ovarian Activity Using the Ovarian Monitor, Part I. Validation of Home and Laboratory Results Obtained During Ovulatory Cycles by Comparison with Radioimmunoassay.” Steroids, 68, no. 5: 465–76. - PubMed
-
- Blackwell L. F., Vigil P., Gross B., d’Arcangues C., Cooke D. G., Brown J. B. 2011. “Monitoring of Ovarian Activity by Measurement of Urinary Excretion Rates of Estrone Glucuronide and Pregnanediol Glucuronide Using the Ovarian Monitor, Part II: Reliability of Home Testing.” Human Reproduction 27: 550–557. doi: 10.1093/humrep/der409. - PubMed
LinkOut - more resources
Full Text Sources