

Ommaya Reservoir Insertion: A Technical Note
- PMID: 32432009
- PMCID: PMC7234073
- DOI: 10.7759/cureus.7731
Ommaya Reservoir Insertion: A Technical Note
Abstract
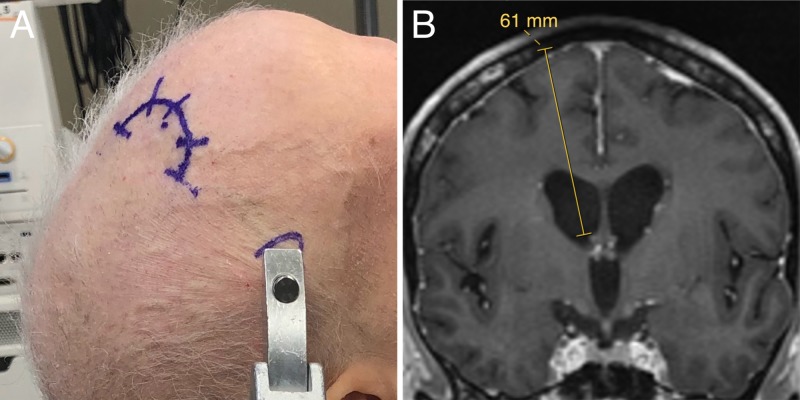
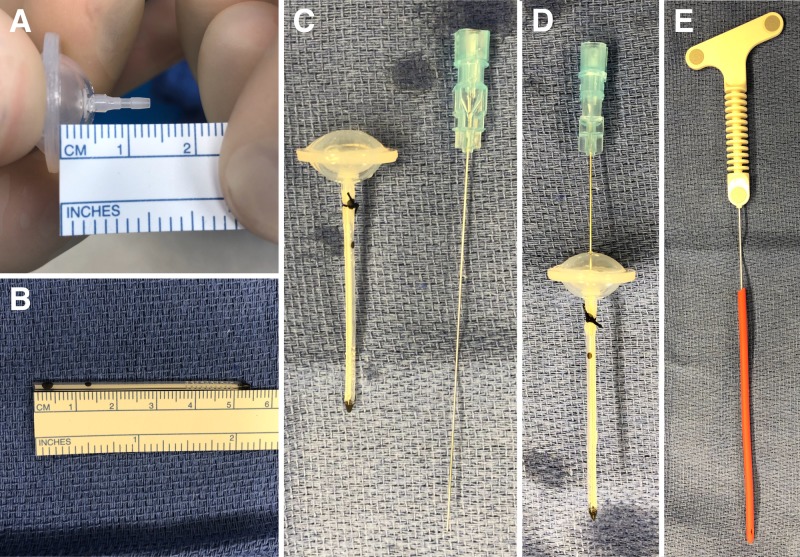
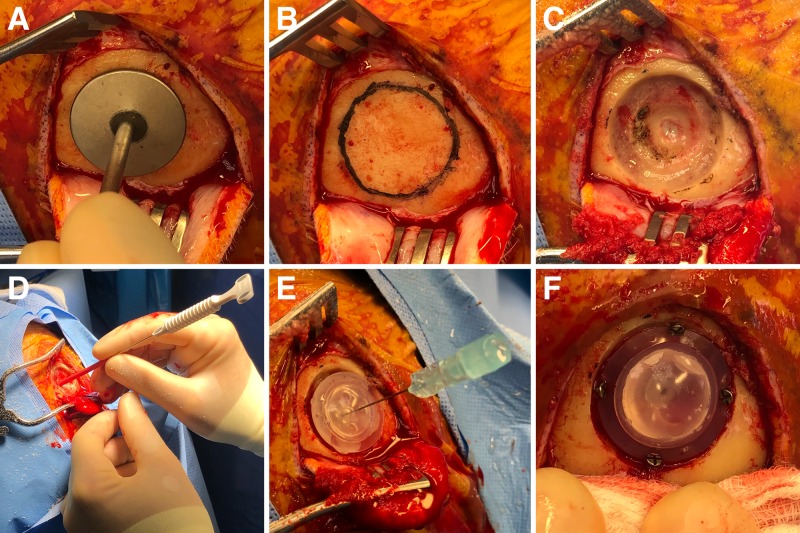
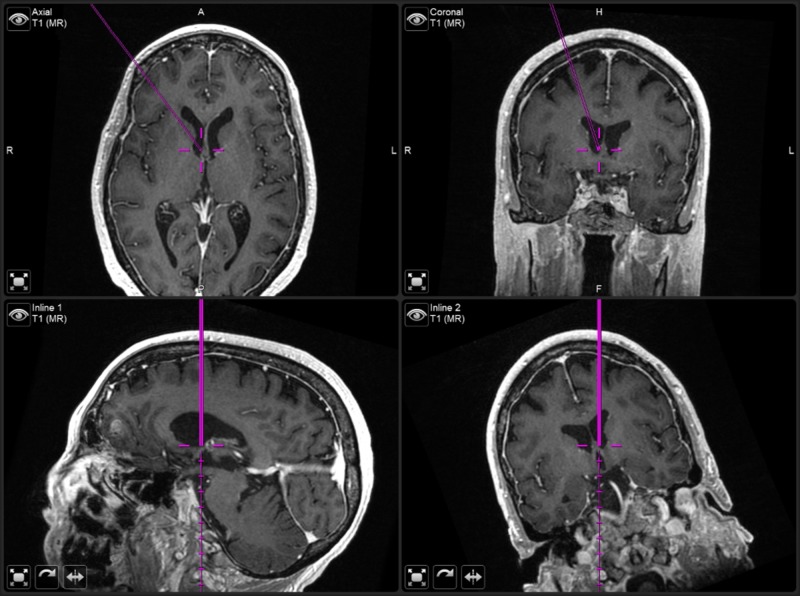
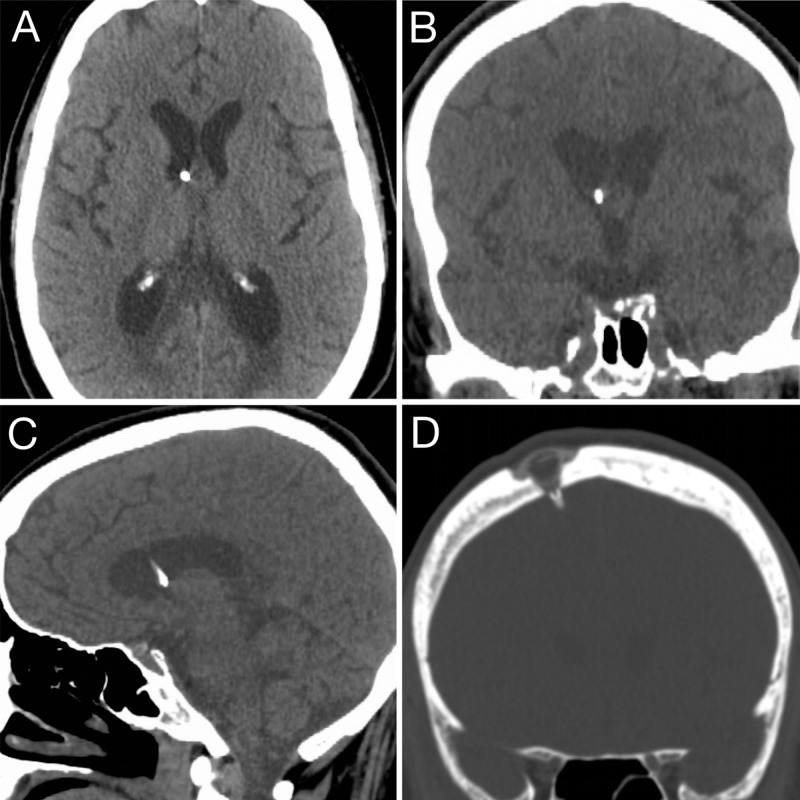
Ommaya reservoir insertion is an elective neurosurgical procedure to deliver repeated intraventricular therapy, but placement can be complicated by malposition of the catheter, clogging, infection or poor postoperative cosmesis. Here, we describe the technique used by the senior author for accurate placement including preassembly of the reservoir and catheter, and recessing of the reservoir so that others may consider the technique for their practice. Results in a consecutive series of 27 Ommaya placements were reviewed. Catheter tip placement accuracy, complications and surgical times were reported. Indications were leptomeningeal cancer or infection. Postoperative imaging showed the catheter tip was located in the frontal horn (96%) or body (4%) of the ipsilateral lateral ventricle. The median surgical time was 36 minutes (range 17-63 minutes). There were no parenchymal or subarachnoid hemorrhages. Infections occurred in 7% (n=2) of cases, and both infections presented greater than 60 days postoperative. In conclusion, we have found that image guidance can optimize accuracy in placement, that preassembly of the reservoir and catheter may be used with a 25-gauge spinal needle stylet to minimize risk of clogging during placement, and that recessing of the reservoir produces the best aesthetic result.
Keywords: chemotherapy; image guidance; intrathecal; intraventricular; ommaya; reservoir.
Copyright © 2020, Magill et al.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
The use of a smartphone-assisted ventricle catheter guide for Ommaya reservoir placement-experience of a retrospective bi-center study.Childs Nerv Syst. 2018 May;34(5):853-859. doi: 10.1007/s00381-017-3713-6. Epub 2018 Jan 10. Childs Nerv Syst. 2018. PMID: 29322340
-
Image-guided Ommaya reservoir insertion for intraventricular chemotherapy: a retrospective series.Acta Neurochir (Wien). 2018 Mar;160(3):539-544. doi: 10.1007/s00701-017-3454-z. Epub 2018 Jan 5. Acta Neurochir (Wien). 2018. PMID: 29305723
-
Navigation-guided Ommaya reservoir placement: implications for the treatment of leptomeningeal metastases.Minim Invasive Neurosurg. 2007 Dec;50(6):340-5. doi: 10.1055/s-2007-993162. Minim Invasive Neurosurg. 2007. PMID: 18210356 Clinical Trial.
-
Placement of the Ommaya reservoir in narrow and slit-like ventricles using a neuronavigation system. Author's own experience and literature review.Zh Vopr Neirokhir Im N N Burdenko. 2014;78(3):38-43. Zh Vopr Neirokhir Im N N Burdenko. 2014. PMID: 25146655 Review. English, Russian.
-
Operative Complications with and without Image Guidance: A Systematic Review and Meta-Analysis of the Ommaya Reservoir Literature.World Neurosurg. 2019 Feb;122:404-414. doi: 10.1016/j.wneu.2018.11.036. Epub 2018 Nov 14. World Neurosurg. 2019. PMID: 30447448
Cited by
-
Fractionated Gamma Knife radiosurgery after cyst aspiration for large cystic brain metastases: case series and literature review.Neurosurg Rev. 2022 Oct;45(5):3457-3465. doi: 10.1007/s10143-022-01835-y. Epub 2022 Jul 14. Neurosurg Rev. 2022. PMID: 35834076 Review.
-
Impact of cerebrospinal fluid flow study in patients undergoing intrathecal chemotherapy via ventricular catheter reservoir.J Neurooncol. 2021 May;153(1):161-167. doi: 10.1007/s11060-021-03756-0. Epub 2021 Apr 15. J Neurooncol. 2021. PMID: 33860429
-
The Emerging Applications of Nanotechnology in Neuroimaging: A Comprehensive Review.Front Bioeng Biotechnol. 2022 Jul 6;10:855195. doi: 10.3389/fbioe.2022.855195. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 35875504 Free PMC article. Review.
-
Integrating Nanotechnology in Neurosurgery, Neuroradiology, and Neuro-Oncology Practice-The Clinicians' Perspective.Front Bioeng Biotechnol. 2022 Feb 9;10:801822. doi: 10.3389/fbioe.2022.801822. eCollection 2022. Front Bioeng Biotechnol. 2022. PMID: 35223783 Free PMC article. No abstract available.
-
Dr Ayub Khan Ommaya (1930-2008): The eventful life of a revolutionary neurosurgeon.J Med Biogr. 2024 Nov;32(4):380-385. doi: 10.1177/09677720231198502. Epub 2023 Sep 18. J Med Biogr. 2024. PMID: 37722807 Free PMC article.
References
-
- Subcutaneous reservoir and pump for sterile access to ventricular cerebrospinal fluid. Ommaya A. Lancet. 1963;282:983–984. - PubMed
-
- Catheter placement for ommaya reservoirs with frameless surgical navigation: technical note. Greenfield JP, Schwartz TH. Stereot Funct Neurosurg. 2007;86:101–105. - PubMed
-
- Ommaya reservoir with ventricular catheter placement for chemotherapy with frameless and pinless electromagnetic surgical neuronavigation. Weiner GM, Chivukula S, Chen C-J, Ding D, Engh JA, Amankulor N. Clin Neurol Neurosurg. 2015;130:61–66. - PubMed
-
- Ommaya reservoir-related infections: clinical manifestations and treatment outcomes. Szvalb AD, Raad II, Weinberg JS, Suki D, Mayer R, Viola GM. J Infect. 2014;68:216–224. - PubMed
LinkOut - more resources
Full Text Sources
Molecular Biology Databases