

Time to Say Goodbye to Bronchiolitis, Viral Wheeze, Reactive Airways Disease, Wheeze Bronchitis and All That
- PMID: 32432064
- PMCID: PMC7214804
- DOI: 10.3389/fped.2020.00218
Time to Say Goodbye to Bronchiolitis, Viral Wheeze, Reactive Airways Disease, Wheeze Bronchitis and All That
Abstract
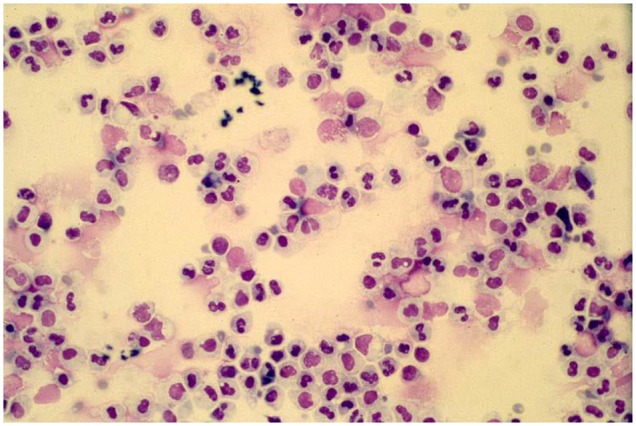
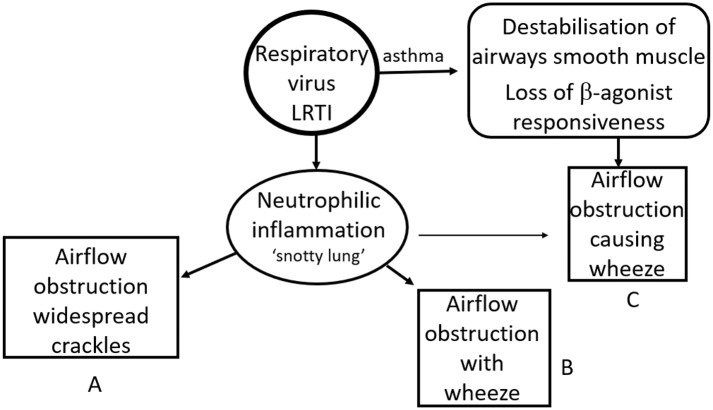
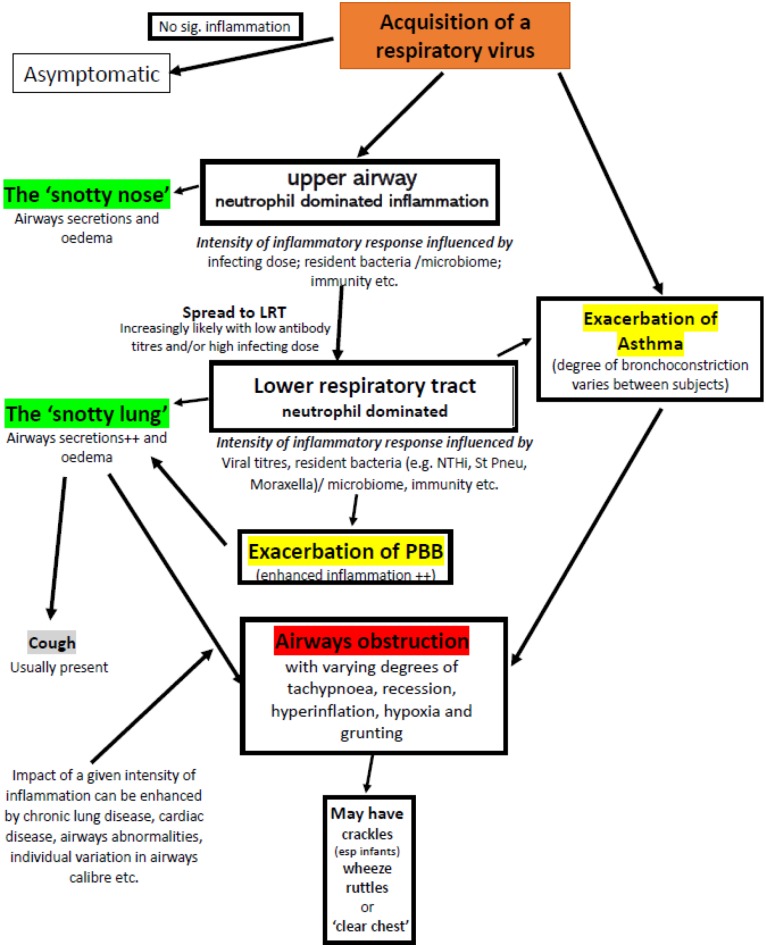
The diagnosis and management of infants and children with a significant viral lower respiratory tract illness remains the subject of much debate and little progress. Over the decades various terms for such illnesses have been in and fallen out of fashion or have evolved to mean different things to different clinicians. Terms such as "bronchiolitis," "reactive airways disease," "viral wheeze," and many more are used to describe the same condition and the same term is frequently used to describe illnesses caused by completely different dominant pathologies. This lack of clarity is due, in large part, to a failure to understand the basic underlying inflammatory and associated processes and, in part, due to the lack of a simple test to identify a condition such as asthma. Moreover, there is a lack of insight into the fact that the same pathology can produce different clinical signs at different ages. The consequence is that terminology and fashions in treatment have tended to go around in circles. As was noted almost 60 years ago, amongst pre-school children with a viral LRTI and airways obstruction there are those with a "viral bronchitis" and those with asthma. In the former group, a neutrophil dominated inflammation response is responsible for the airways' obstruction whilst amongst asthmatics much of the obstruction is attributable to bronchoconstriction. The airways obstruction in the former group is predominantly caused by airways secretions and to some extent mucosal oedema (a "snotty lung"). These patients benefit from good supportive care including supplemental oxygen if required (though those with a pre-existing bacterial bronchitis will also benefit from antibiotics). For those with a viral exacerbation of asthma, characterized by bronchoconstriction combined with impaired b-agonist responsiveness, standard management of an exacerbation of asthma (including the use of steroids to re-establish bronchodilator responsiveness) represents optimal treatment. The difficulty is identifying which group a particular patient falls into. A proposed simplified approach to the nomenclature used to categorize virus associated LRTIs is presented based on an understanding of the underlying pathological processes and how these contribute to the physical signs.
Keywords: diagnostic feature; infant; lower respiratory tract infection; neutrophil; pre-school age children; viral; wheeze.
Copyright © 2020 Douros and Everard.
Figures
Similar articles
-
Management of Recurrent Preschool, Doctor-Diagnosed Wheeze.Indian J Pediatr. 2018 Aug;85(8):658-666. doi: 10.1007/s12098-017-2537-4. Epub 2018 Jan 8. Indian J Pediatr. 2018. PMID: 29308548 Review.
-
Role of viral infections in the development and exacerbation of asthma in children.J Allergy Clin Immunol. 2017 Oct;140(4):895-906. doi: 10.1016/j.jaci.2017.08.003. J Allergy Clin Immunol. 2017. PMID: 28987219 Free PMC article. Review.
-
'Recurrent lower respiratory tract infections' - going around in circles, respiratory medicine style.Paediatr Respir Rev. 2012 Sep;13(3):139-43. doi: 10.1016/j.prrv.2012.03.003. Epub 2012 Apr 11. Paediatr Respir Rev. 2012. PMID: 22726868 Review.
-
Association of Rhinovirus C Bronchiolitis and Immunoglobulin E Sensitization During Infancy With Development of Recurrent Wheeze.JAMA Pediatr. 2019 Jun 1;173(6):544-552. doi: 10.1001/jamapediatrics.2019.0384. JAMA Pediatr. 2019. PMID: 30933255 Free PMC article.
-
Infants Hospitalized with Lower Respiratory Tract Infections Were More Likely to Develop Asthma.Adv Respir Med. 2022 Jul 21;90(4):246-253. doi: 10.3390/arm90040034. Adv Respir Med. 2022. PMID: 35892745 Free PMC article.
Cited by
-
Patterns of respiratory health services utilization from birth to 5 years of children who experienced adverse birth outcomes.PLoS One. 2021 Feb 19;16(2):e0247527. doi: 10.1371/journal.pone.0247527. eCollection 2021. PLoS One. 2021. PMID: 33606848 Free PMC article.
-
Association between socioeconomic deprivation, ethnicity and health outcomes in preschool children with recurrent wheeze in England: a retrospective cohort study.Thorax. 2024 Oct 16;79(11):1050-1059. doi: 10.1136/thorax-2023-221210. Thorax. 2024. PMID: 38955499 Free PMC article.
-
Smart Devices Are Poised to Revolutionize the Usefulness of Respiratory Sounds.Chest. 2023 Jun;163(6):1519-1528. doi: 10.1016/j.chest.2023.01.024. Epub 2023 Jan 25. Chest. 2023. PMID: 36706908 Free PMC article. Review.
-
Pneumonia in Infancy and Risk for Asthma: The Role of Familial Confounding and Pneumococcal Vaccination.Chest. 2021 Aug;160(2):422-431. doi: 10.1016/j.chest.2021.03.006. Epub 2021 Mar 13. Chest. 2021. PMID: 33727032 Free PMC article.
-
Bronchiolitis recovery and the use of High Efficiency Particulate Air (HEPA) Filters (The BREATHE Study): study protocol for a multi-center, parallel, double-blind, randomized controlled clinical trial.Trials. 2024 Mar 20;25(1):197. doi: 10.1186/s13063-024-08012-0. Trials. 2024. PMID: 38504367 Free PMC article.
References
-
- Tyrell DA. Discovering and defining the etiology of acute viral respiratory viral disease. Am Rev Respir Dis. (1963) 88(Suppl.):77–88. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical
Research Materials