

Infectious Complications Following CD19 Chimeric Antigen Receptor T-cell Therapy for Children, Adolescents, and Young Adults
- PMID: 32432149
- PMCID: PMC7221263
- DOI: 10.1093/ofid/ofaa121
Infectious Complications Following CD19 Chimeric Antigen Receptor T-cell Therapy for Children, Adolescents, and Young Adults
Abstract
Background: Infectious complications of chimeric antigen receptor (CAR) T-cell immunotherapy in children and young adults have not been well described.
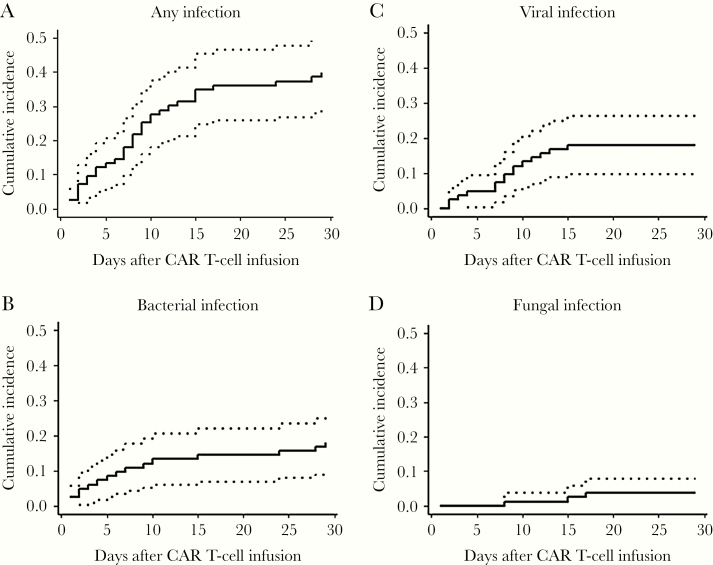
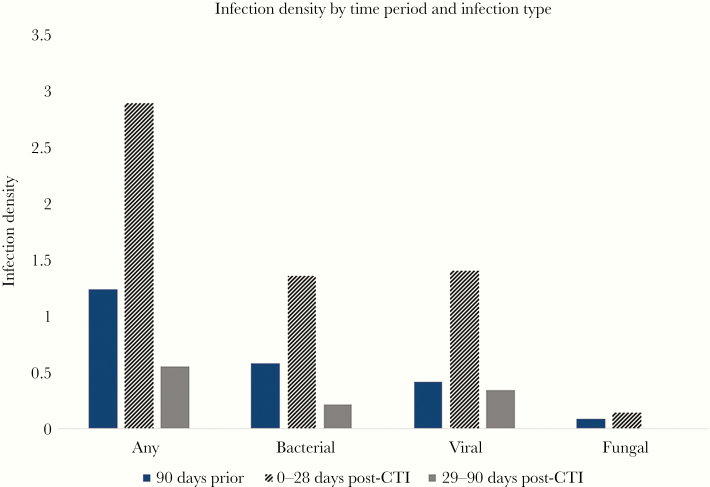
Methods: Medical records of patients ≤26 years old receiving CD19 CAR T-cell infusion (CTI) at a single institution between 2014 and 2017 were reviewed. The number of infections per 100 days-at-risk (infection density) in the 90 days preceding and 0-28 and 29-90 days after CTI was calculated. Poisson regression and Cox analyses were utilized to identify risk factors for infections.
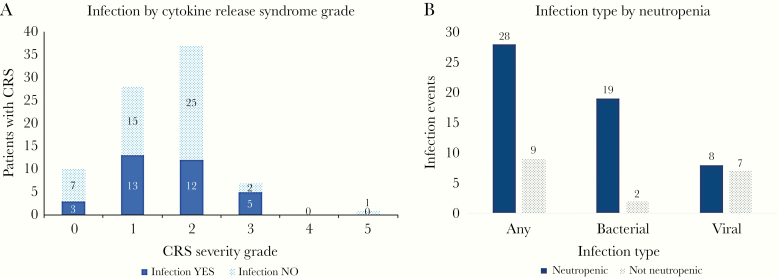
Results: Eighty-three patients received CTI during the study period. Most patients (98%) had refractory or relapsed acute lymphoblastic leukemia (ALL). Infections occurred in 54% of patients in the 90 days before CTI (infection density, 1.23) and in 40% of patients in the first 28 days following CTI (infection density, 2.89). Infection density decreased to 0.55 in the 29-90 days post-CTI. Most infections were bacteremias (39%) or respiratory viral infections (43%). Pre-CTI risk factors associated with infection included prior hematopoietic cell transplantation (HCT), immunoglobulin G (IgG) level <400 mg/dL, and lymphodepletion other than cyclophosphamide plus fludarabine; post-CTI risk factors included higher-severity CRS and IgG <400 mg/dL.
Conclusions: Infection rates in children and young adults receiving CD19 CAR T-cell therapy increase in the first month and then decline. Understanding types and timing of infections and contributing risk factors may help inform prophylactic and monitoring strategies. Specific attention should be given to patients with prior HCT, severe hypogammaglobulinemia, and severe CRS.
Keywords: ALL; CAR T-cell; immunotherapy; infection; pediatric.
© The Author(s) 2020. Published by Oxford University Press on behalf of Infectious Diseases Society of America.
Figures
References
-
- FDA approval brings first gene therapy to the United States. 2017. Available at: https://www.fda.gov/news-events/press-announcements/fda-approval-brings-.... Accessed February 1, 2020.
