

Prognostic significance of right ventricular hypertrophy and systolic function in Anderson-Fabry disease
- PMID: 32432376
- PMCID: PMC7373914
- DOI: 10.1002/ehf2.12712
Prognostic significance of right ventricular hypertrophy and systolic function in Anderson-Fabry disease
Abstract
Aims: Right ventricular hypertrophy (RVH) is a common finding in Anderson-Fabry disease (AFD), but the prognostic role of right ventricular (RV) involvement has never been assessed. The aim of our study was to evaluate the prognostic significance of RVH and RV systolic function in AFD.
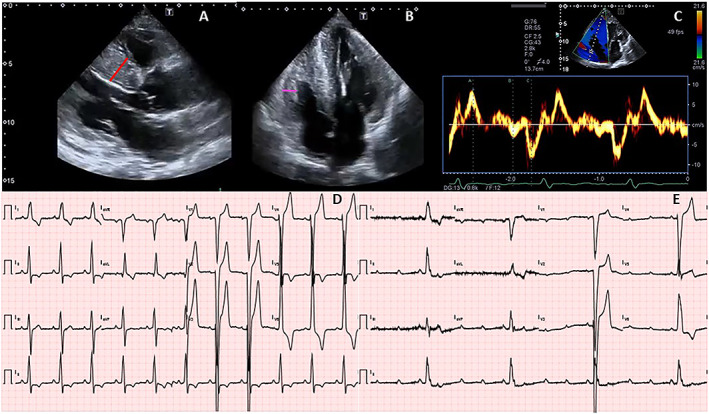
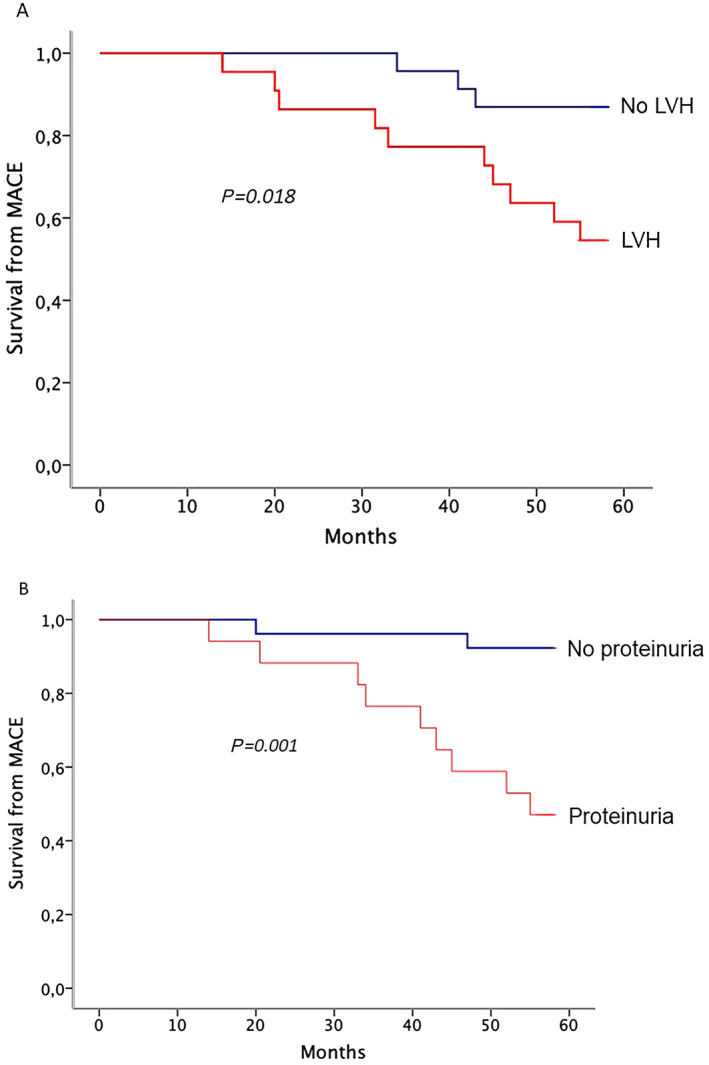
Methods and results: Forty-five AFD patients (56% male patients) with extensive baseline evaluation, including assessment of RVH and RV systolic function, were followed-up for an average of 51.2 ± 11.4 months. RV systolic function was assessed by standard and tissue Doppler echocardiography. Cardiovascular events were defined as new-onset atrial fibrillation (AF), sustained ventricular arrhythmias, heart failure, or pacemaker/implantable cardioverter defibrillator implantation; renal events were defined as progression to dialysis and/or renal transplantation or significant worsening of glomerular filtration rate; and cerebrovascular events were defined as transient ischaemic attack or stroke. Fourteen patients (31.1%) presented RVH, while RV systolic function was normal in all cases. During the follow-up period, 13 patients (28.8%, 11 male) experienced 18 major events, including two deaths. Cardiovascular events occurred in eight patients (17.7%). The most common event was pacemaker/implantable cardioverter defibrillator implantation (six patients, 13.3%), followed by AF (three cases, 6.6%). Only one case of worsening New York Heart Association class (from II to III and IV) was observed. Ischaemic stroke occurred in three cases (6.6%). Renal events were recorded in three patients (6.6%). At univariate analysis, several variables were associated with the occurrence of events, including RVH (HR: 7.09, 95% CI: 2.17 to 23.14, P = 0.001) and indexes of RV systolic function (tricuspid annular plane systolic excursion HR: 0.77, 95% CI: 0.62 to 0.96, P = 0.02; and RV tissue Doppler systolic velocity HR: 0.76, 95% CI: 0.61 to 0.93, P = 0.01). At multivariate analysis, proteinuria (HR:8.3, 95% CI: 2.88 to 23.87, P < 0.001) and left ventricular mass index (HR: 1.02, 95% CI: 1.00 to 1.03, P = 0.03) emerged as the only independent predictors of outcome.
Conclusions: RVH and RV systolic function show significant association with clinical events in AFD, but only proteinuria and left ventricular mass index emerged as independent predictors of outcome. Our findings suggest that RV involvement does not influence prognosis in AFD and confirm that renal involvement and left ventricular hypertrophy are the main determinant of major cardiac and non-cardiac events.
Keywords: Anderson-Fabry disease; Prognosis; RV systolic function; RVH.
© 2020 The Authors. ESC Heart Failure published by John Wiley & Sons Ltd on behalf of the European Society of Cardiology.
Conflict of interest statement
Francesca Graziani: honoraria for board meetings and travel support from Amicus Therapeutics, Sanofi‐Genzyme, and Shire. Antonia Camporeale: honoraria for presentations and board meetings from Amicus Therapeutics, Sanofi‐Genzyme, and Shire; and research grant from Amicus Therapeutics. Maurizio Pieroni: speaker and advisory board honoraria and travel support from Sanofi‐Genzyme, Amicus Therapeutics, and Shire. Rosa Lillo: honoraria for board meetings and travel support from Amicus Therapeutics and Shire.
Figures
References
-
- Brady RO, Gal AE, Bradley RM, Martensson E, Warshaw AL, Laster L. Enzymatic defect in Fabry's disease: ceramidetrihexosidase deficiency. N Engl J Med 1967; 276: 1163–1167. - PubMed
-
- Sheppard MN, Cane P, Florio R, Kavantzas N, Close L, Shah J, Lee P, Elliott P. A detailed pathologic examination of heart tissue from three older patients with Anderson‐Fabry disease on enzyme replacement therapy. Cardiovasc Pathol 2010; 19: 293–301. - PubMed
-
- Kampmann C, Baehner FA, Whybra C, Bajbouj M, Baron K, Knuf M, Wiethoff CM, Trübel H, Beck M. The right ventricle in Fabry disease. Acta Paediatric Int J Paediatric Supp 2005; 94: 15–18. - PubMed
-
- Palecek T, Dostalova G, Kuchynka P, Karetova D, Bultas J, Elleder M, Linhart A. Right ventricular involvement in Fabry disease. J Am Soc Echocardiogr 2008; 21: 1265–1268. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Medical