

Complete vs Culprit-Lesion-Only Revascularization for ST-Segment Elevation Myocardial Infarction: A Systematic Review and Meta-analysis
- PMID: 32432651
- PMCID: PMC7240651
- DOI: 10.1001/jamacardio.2020.1251
Complete vs Culprit-Lesion-Only Revascularization for ST-Segment Elevation Myocardial Infarction: A Systematic Review and Meta-analysis
Abstract
Importance: Recently, the Complete vs Culprit-Only Revascularization to Treat Multivessel Disease After Early PCI (percutaneous coronary intervention) for STEMI (ST-segment elevation myocardial infarction [MI]) (COMPLETE) trial showed that angiography-guided PCI of the nonculprit lesion with the goal of complete revascularization reduced cardiovascular (CV) death or new MI compared with PCI of the culprit lesion only in STEMI. Whether complete revascularization also reduces CV mortality is uncertain. Moreover, whether the association of complete revascularization with hard clinical outcomes is consistent when fractional flow reserve (FFR)- and angiography-guided strategies are used is unknown.
Objective: To determine through a systematic review and meta-analysis (1) whether complete revascularization is associated with decreased CV mortality and (2) whether heterogeneity in the association occurs when FFR- and angiography-guided PCI strategies for nonculprit lesions are performed.
Data sources: A systematic search of MEDLINE, Embase, ISI Web of Science, and CENTRAL (Cochrane Central Register of Controlled Trials) from database inception to September 30, 2019, was performed. Conference proceedings were also reviewed from January 1, 2002, to September 30, 2019.
Study selection: English-language randomized clinical trials comparing complete revascularization vs culprit-lesion-only PCI in patients with STEMI and multivessel disease were included.
Data extraction and synthesis: The combined odds ratio (OR) was calculated with the random-effects model using the Mantel-Haenszel method (sensitivity with fixed-effects model). Heterogeneity was measured using the I2 statistic. Publication bias was evaluated using the inverted funnel plot approach. Data were analyzed from October 2019 to January 2020.
Main outcomes and measures: Cardiovascular death and the composite of CV death or new MI.
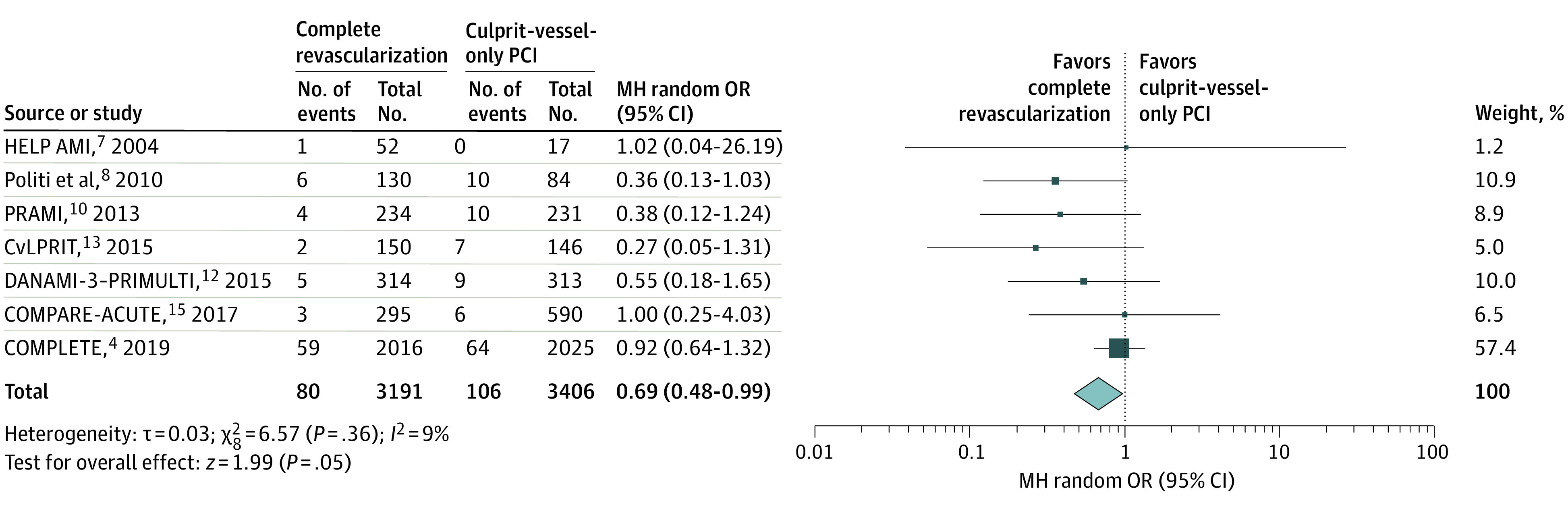
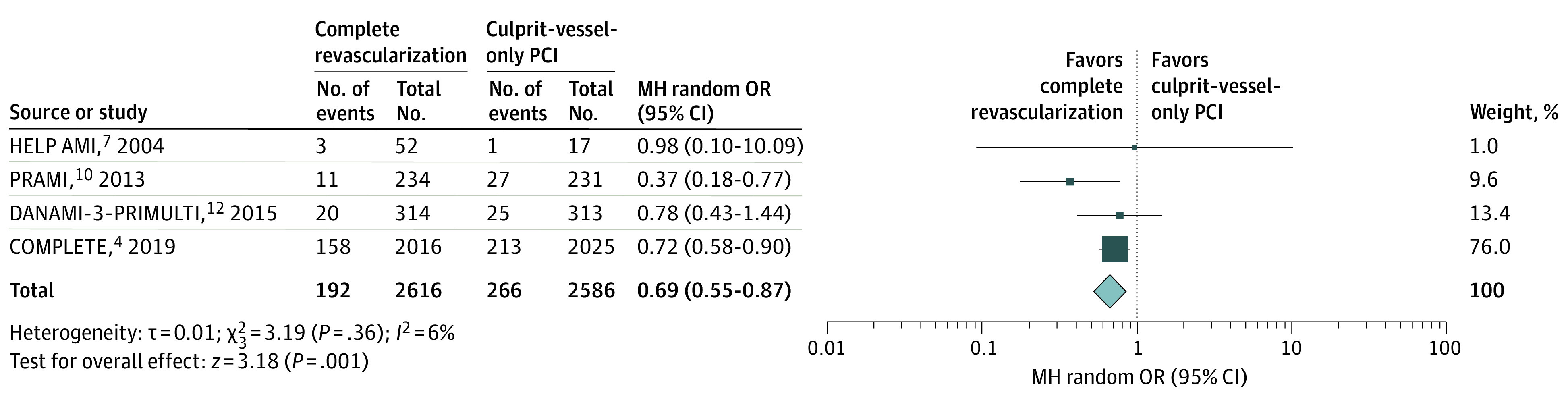
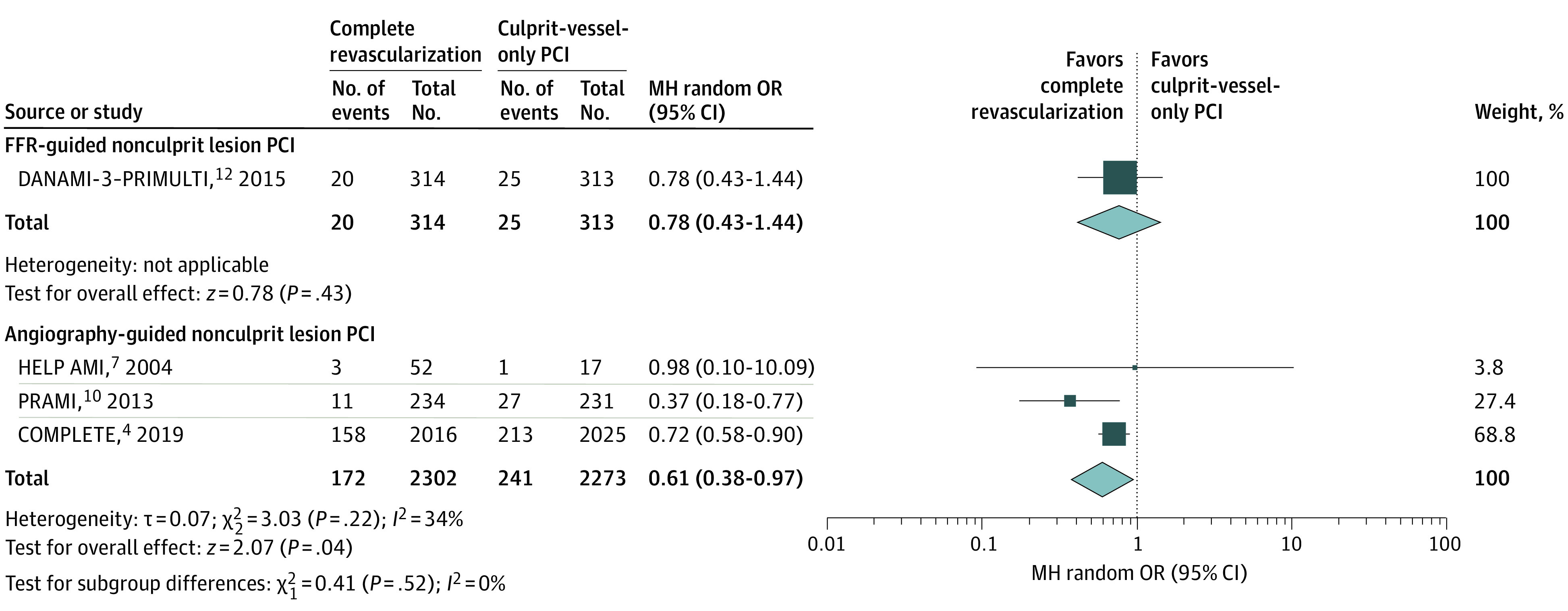
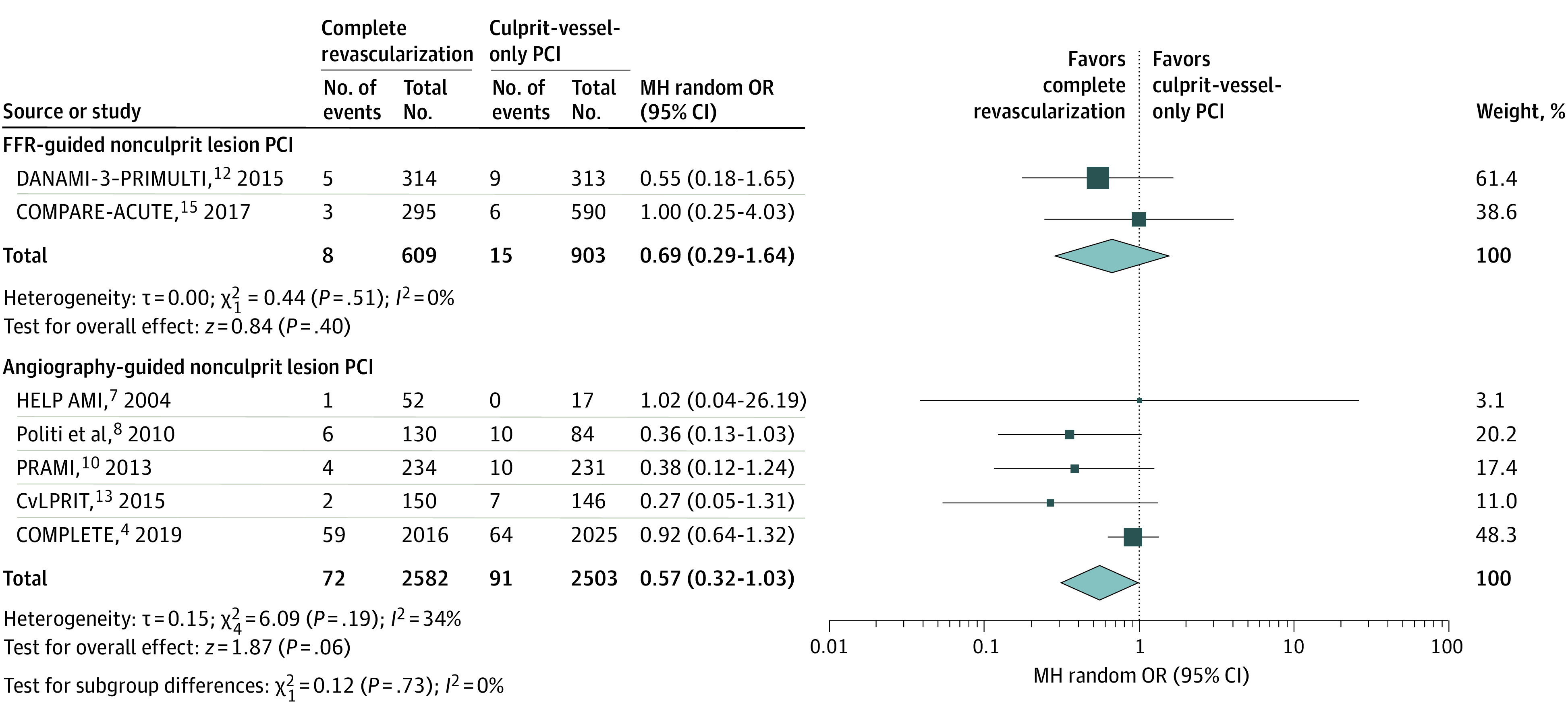
Results: Ten randomized clinical trials involving 7030 unique patients were included. The weighted mean follow-up time was 29.5 months. Complete revascularization was associated with reduced CV death compared with culprit-lesion-only PCI (80 of 3191 [2.5%] vs 106 of 3406 [3.1%]; OR, 0.69 [95% CI, 0.48-0.99]; P = .05; fixed-effects model OR, 0.74 [95% CI, 0.55-0.99]; P = .04). All-cause mortality occurred in 153 of 3426 patients (4.5%) in the complete revascularization group vs 177 of 3604 (4.9%) in the culprit-lesion-only group (OR, 0.84 [95% CI, 0.67-1.05]; P = .13; I2 = 0%). Complete revascularization was associated with a reduced composite of CV death or new MI (192 of 2616 [7.3%] vs 266 of 2586 [10.3%]; OR, 0.69 [95% CI, 0.55-0.87]; P = .001; fixed-effects model OR, 0.69 [95% CI, 0.57-0.84]; P < .001), with no heterogeneity in this outcome when complete revascularization was performed using an FFR-guided strategy (OR, 0.78 [95% CI, 0.43-1.44]) or an angiography-guided strategy (OR, 0.61 [95% CI, 0.38-0.97]; P = .52 for interaction).
Conclusions and relevance: In patients with STEMI and multivessel disease, complete revascularization was associated with a reduction in CV mortality compared with culprit-lesion-only PCI. There was no differential association with treatment between FFR- and angiography-guided strategies on major CV outcomes.
Conflict of interest statement
Figures
References
-
- Ibanez B, James S, Agewall S, et al. ; ESC Scientific Document Group . 2017 ESC guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the task force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119-177. doi:10.1093/eurheartj/ehx393 - DOI - PubMed
-
- Levine GN, Bates ER, Blankenship JC, et al. . 2015 ACC/AHA/SCAI focused update on primary percutaneous coronary intervention for patients with ST-elevation myocardial infarction: an update of the 2011 ACCF/AHA/SCAI guideline for percutaneous coronary intervention and the 2013 ACCF/AHA guideline for the management of ST-elevation myocardial infarction: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Society for Cardiovascular Angiography and Interventions. Circulation. 2016;133(11):1135-1147. doi:10.1161/CIR.0000000000000336 - DOI - PubMed
-
- Higgins JPT, Green S, eds. Cochrane Handbook for Systematic Reviews of Interventions, Version 5.1.0 [updated March 2011]. The Cochrane Collaboration; 2011. https://training.cochrane.org/handbook
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
