

Technologies to Optimize the Care of Severe COVID-19 Patients for Health Care Providers Challenged by Limited Resources
- PMID: 32433248
- PMCID: PMC7258840
- DOI: 10.1213/ANE.0000000000004985
Technologies to Optimize the Care of Severe COVID-19 Patients for Health Care Providers Challenged by Limited Resources
Abstract
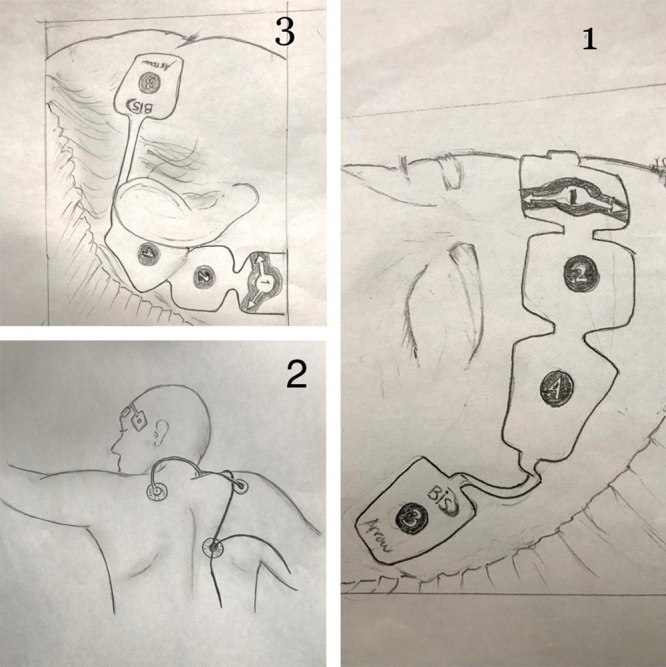
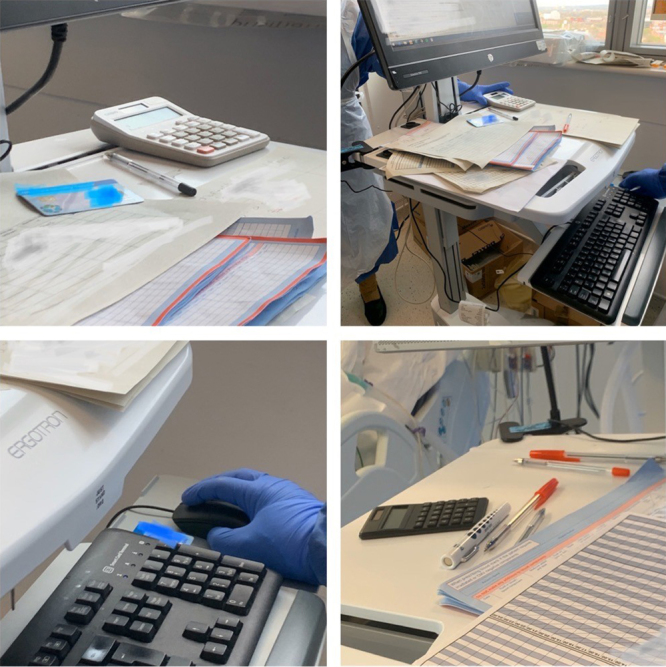
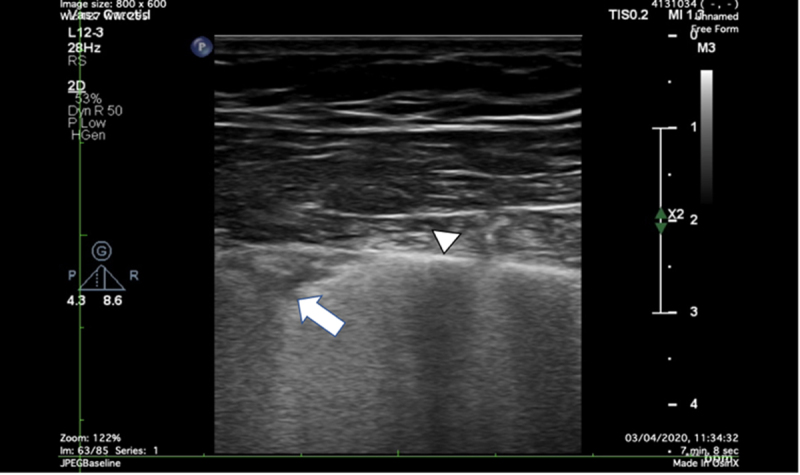
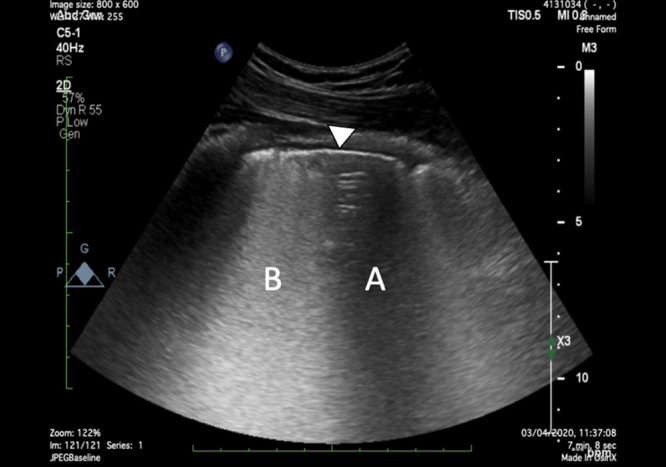
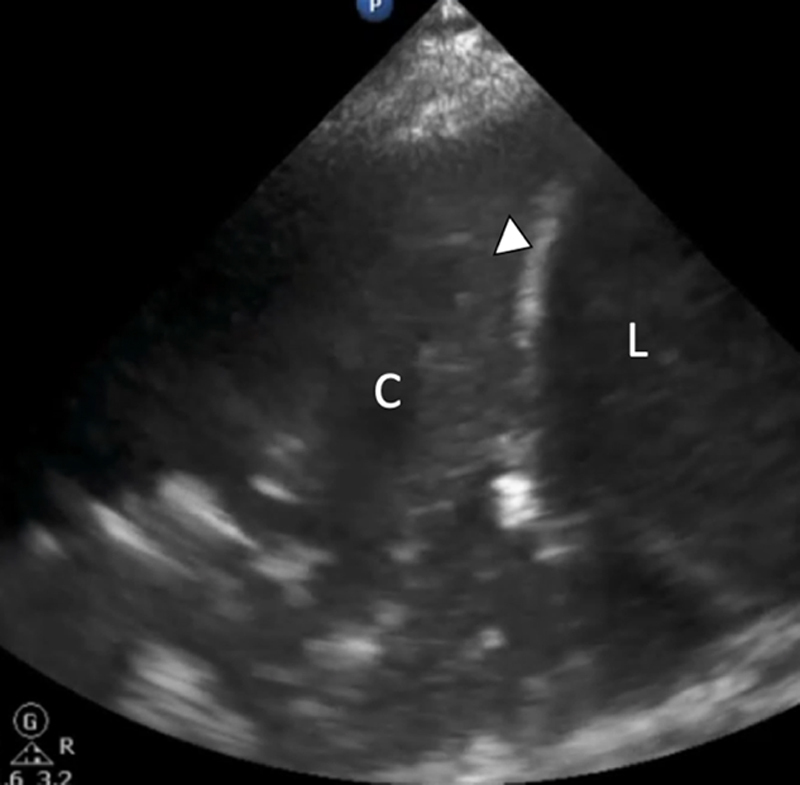
Health care systems are belligerently responding to the new coronavirus disease 2019 (COVID-19). The severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) is a specific condition, whose distinctive features are severe hypoxemia associated with (>50% of cases) normal respiratory system compliance. When a patient requires intubation and invasive ventilation, the outcome is poor, and the length of stay in the intensive care unit (ICU) is usually 2 or 3 weeks. In this article, the authors review several technological devices, which could support health care providers at the bedside to optimize the care for COVID-19 patients who are sedated, paralyzed, and ventilated. Particular attention is provided to the use of videolaryngoscopes (VL) because these can assist anesthetists to perform a successful intubation outside the ICU while protecting health care providers from this viral infection. Authors will also review processed electroencephalographic (EEG) monitors which are used to better titrate sedation and the train-of-four monitors which are utilized to better administer neuromuscular blocking agents in the view of sparing limited pharmacological resources. COVID-19 can rapidly exhaust human and technological resources too within the ICU. This review features a series of technological advancements that can significantly improve the care of patients requiring isolation. The working conditions in isolation could cause gaps or barriers in communication, fatigue, and poor documentation of provided care. The available technology has several advantages including (a) facilitating appropriate paperless documentation and communication between all health care givers working in isolation rooms or large isolation areas; (b) testing patients and staff at the bedside using smart point-of-care diagnostics (SPOCD) to confirm COVID-19 infection; (c) allowing diagnostics and treatment at the bedside through point-of-care ultrasound (POCUS) and thromboelastography (TEG); (d) adapting the use of anesthetic machines and the use of volatile anesthetics. Implementing technologies for safeguarding health care providers as well as monitoring the limited pharmacological resources are paramount. Only by leveraging new technologies, it will be possible to sustain and support health care systems during the expected long course of this pandemic.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures

Comment in
-
Clarifications on Technologies to Optimize Care of Severe COVID-19 Patients.Anesth Analg. 2020 Oct;131(4):e192-e193. doi: 10.1213/ANE.0000000000005120. Anesth Analg. 2020. PMID: 32665462 Free PMC article. No abstract available.
-
In Response.Anesth Analg. 2020 Oct;131(4):e193-e195. doi: 10.1213/ANE.0000000000005121. Anesth Analg. 2020. PMID: 32665463 Free PMC article. No abstract available.
References
-
- ICNARC COVID-19 report 2020-04-04. Source: ICNARC COVID-19 Study case mix programme database 4th April 2020.
-
- Last JM. A Dictionary of Epidemiology. 20014th ed New York: Oxford University Press
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
