

The emerging spectrum of cardiopulmonary pathology of the coronavirus disease 2019 (COVID-19): Report of 3 autopsies from Houston, Texas, and review of autopsy findings from other United States cities
- PMID: 32434133
- PMCID: PMC7204762
- DOI: 10.1016/j.carpath.2020.107233
The emerging spectrum of cardiopulmonary pathology of the coronavirus disease 2019 (COVID-19): Report of 3 autopsies from Houston, Texas, and review of autopsy findings from other United States cities
Abstract
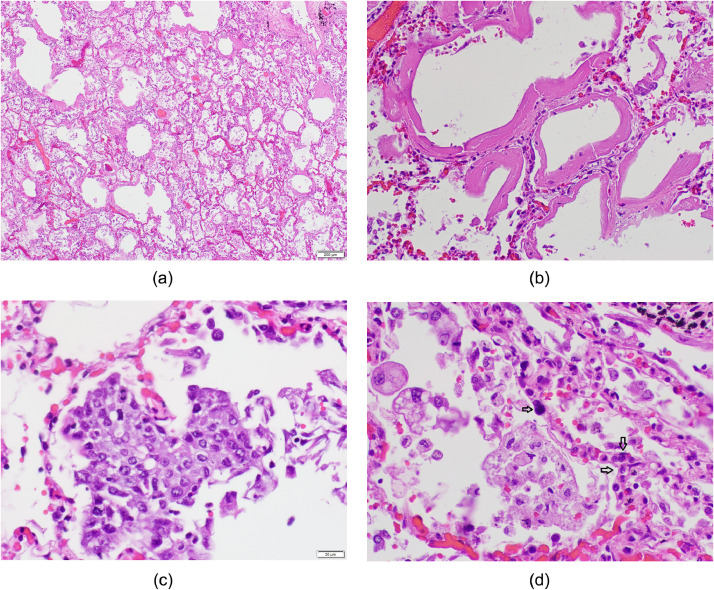
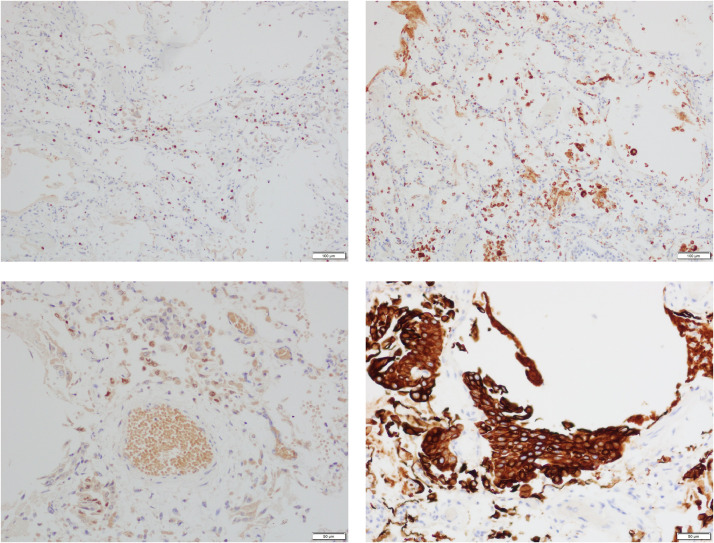
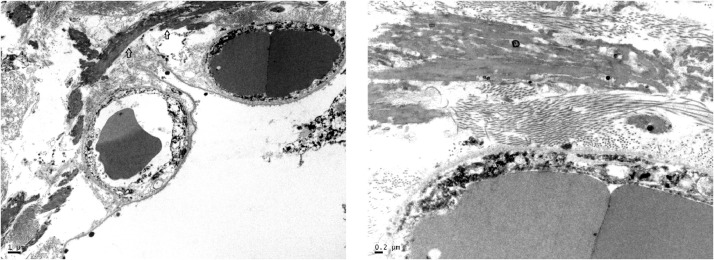
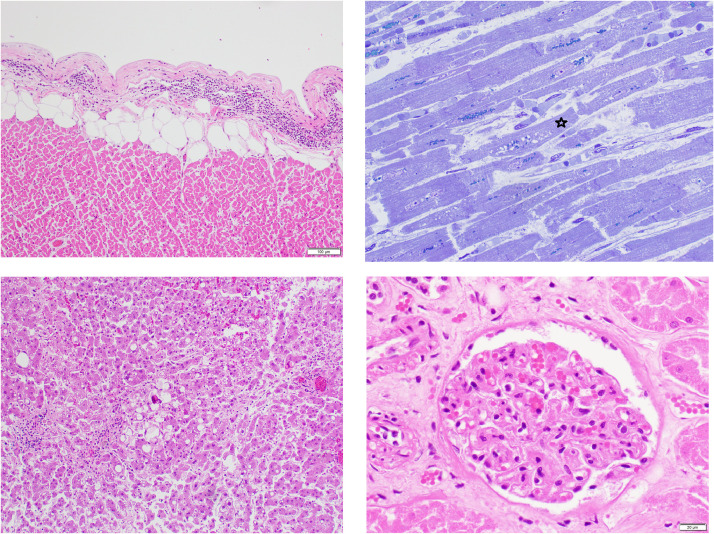
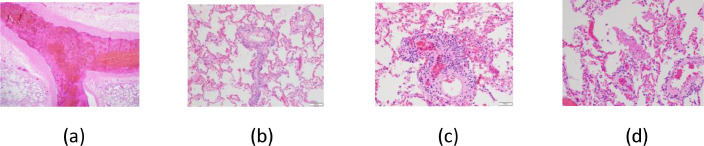
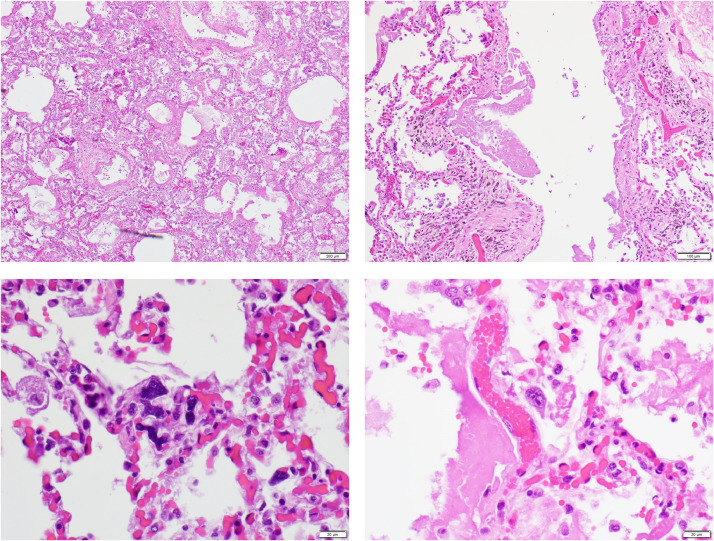
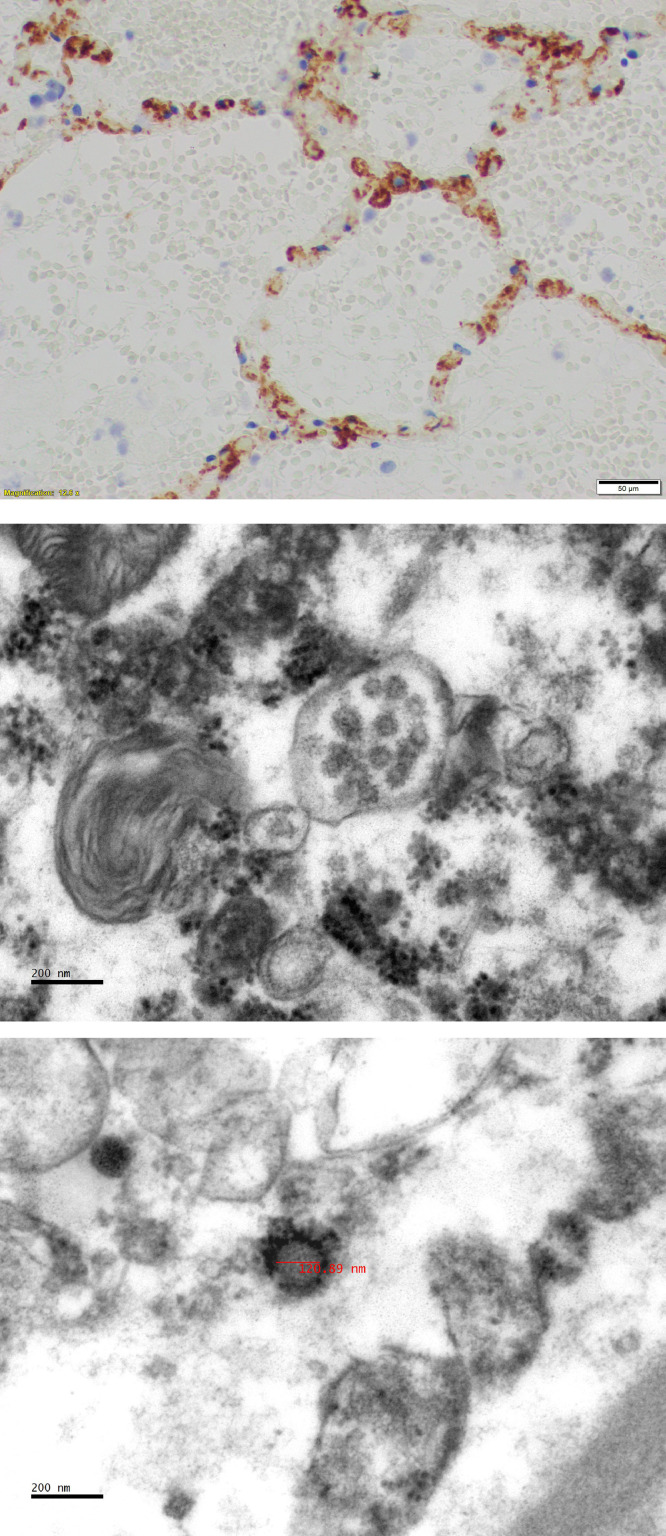
This paper collates the pathological findings from initial published autopsy reports on 23 patients with coronavirus disease 2019 (COVID-19) from 5 centers in the United States of America, including 3 cases from Houston, Texas. Findings confirm that COVID-19 is a systemic disease with major involvement of the lungs and heart. Acute COVID-19 pneumonia has features of a distinctive acute interstitial pneumonia with a diffuse alveolar damage component, coupled with microvascular involvement with intra- and extravascular fibrin deposition and intravascular trapping of neutrophils, and, frequently, with formation of microthombi in arterioles. Major pulmonary thromboemboli with pulmonary infarcts and/or hemorrhage occurred in 5 of the 23 patients. Two of the Houston cases had interstitial pneumonia with diffuse alveolar damage pattern. One of the Houston cases had multiple bilateral segmental pulmonary thromboemboli with infarcts and hemorrhages coupled with, in nonhemorrhagic areas, a distinctive interstitial lymphocytic pneumonitis with intra-alveolar fibrin deposits and no hyaline membranes, possibly representing a transition form to acute fibrinous and organizing pneumonia. Multifocal acute injury of cardiac myocytes was frequently observed. Lymphocytic myocarditis was reported in 1 case. In addition to major pulmonary pathology, the 3 Houston cases had evidence of lymphocytic pericarditis, multifocal acute injury of cardiomyocytes without inflammatory cellular infiltrates, depletion of splenic white pulp, focal hepatocellular degeneration and rare glomerular capillary thrombosis. Each had evidence of chronic cardiac disease: hypertensive left ventricular hypertrophy (420 g heart), dilated cardiomyopathy (1070 g heart), and hypertrophic cardiomyopathy (670 g heart). All 3 subjects were obese (BMIs of 33.8, 51.65, and 35.2 Kg/m2). Overall, the autopsy findings support the concept that the pathogenesis of severe COVID-19 disease involves direct viral-induced injury of multiple organs, including heart and lungs, coupled with the consequences of a procoagulant state with coagulopathy.
Keywords: Autopsy; COVID-19; Coagulopathy; Diffuse alveolar damage; Heart; Kidney; Liver; SARS-CoV-2; Spleen; Viral pneumonia.
Copyright © 2020 Elsevier Inc. All rights reserved.
Conflict of interest statement
Declaration of Competing Interest None.
Figures



Comment in
-
Letter to the editor in response to Buja et al. 2020.Cardiovasc Pathol. 2021 Jan-Feb;50:107269. doi: 10.1016/j.carpath.2020.107269. Epub 2020 Aug 29. Cardiovasc Pathol. 2021. PMID: 32871258 Free PMC article. No abstract available.
-
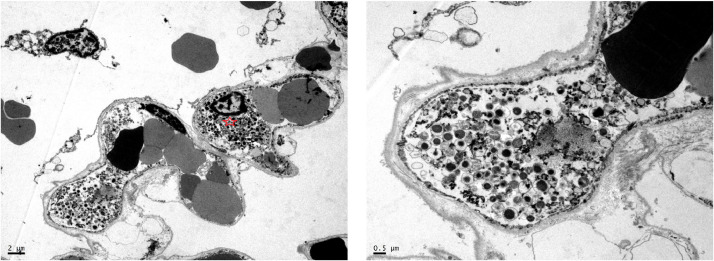
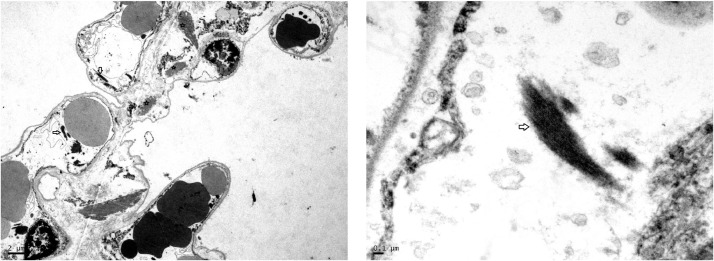
Electron microscopy identification of SARS-COV-2: what is the evidence?Cardiovasc Pathol. 2021 May-Jun;52:107338. doi: 10.1016/j.carpath.2021.107338. Epub 2021 Apr 20. Cardiovasc Pathol. 2021. PMID: 33892096 Free PMC article. No abstract available.
-
Commentary on the spectrum of cardiopulmonary pathology in COVID-19.Cardiovasc Pathol. 2021 Jul-Aug;53:107339. doi: 10.1016/j.carpath.2021.107339. Epub 2021 May 13. Cardiovasc Pathol. 2021. PMID: 33992734 Free PMC article. No abstract available.
References
-
- Wuhan Municipal Health Commission. [Report of clustering pneumonia of unknown etiology in Wuhan City] (In Chinese). Available at: http://wjw.wuhan.gov.cn/front/web/showDetail/2019123108989; 2019Accessed April 15, 2020.
-
- World Health Organization (WHO). Pneumonia of unknown cause – China2020. Available at: https://www.who.int/csr/don/05-january-2020-pneumonia-of-unkown-cause-ch...; Accessed April 15, 2020.
-
- Scherer A. Golden Helix; 2020. Genetic analysis of the covid-19 virus and other pathogens.https://www.goldenhelix.com/resources/ebooks/genetic-analysis-covid-19-o... Available at. Accessed April 15, 2020.
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
