

GlideScope® versus C-MAC®(D) videolaryngoscope versus Macintosh laryngoscope for double lumen endotracheal intubation in patients with predicted normal airways: a randomized, controlled, prospective trial
- PMID: 32434470
- PMCID: PMC7238523
- DOI: 10.1186/s12871-020-01012-y
GlideScope® versus C-MAC®(D) videolaryngoscope versus Macintosh laryngoscope for double lumen endotracheal intubation in patients with predicted normal airways: a randomized, controlled, prospective trial
Abstract
Background: The double lumen endotracheal tube (DLT) is the most widely-used device for single lung ventilation in current thoracic anesthesia practice. In recent years, the routine application of the videolaryngoscope for single lumen endotracheal intubation has increased; nevertheless there are few studies of the use of the videolaryngoscope for DLT. We wondered whether there were benefits to using the videolaryngoscope for DLT placement in patients with predicted normal airways. Therefore, this study was designed to compare the performances of the GlideScope®, the C-MAC®(D) videolaryngoscope and the Macintosh laryngoscope in DLT intubation.
Methods: This was a randomized, controlled, prospective study. We randomly allocated 90 adult patients with predicted normal airways into three groups. All patients underwent routine anesthesia using different laryngoscopes according to group allocation. We compared DLT insertion times, first-pass success rates, numerical rating scales (NRS) of DLT delivery and DLT insertion, Cormack-Lehane degrees (C/L), hemodynamic changes and incidences of intubation complications. All outcomes were analyzed using SPSS13.0.
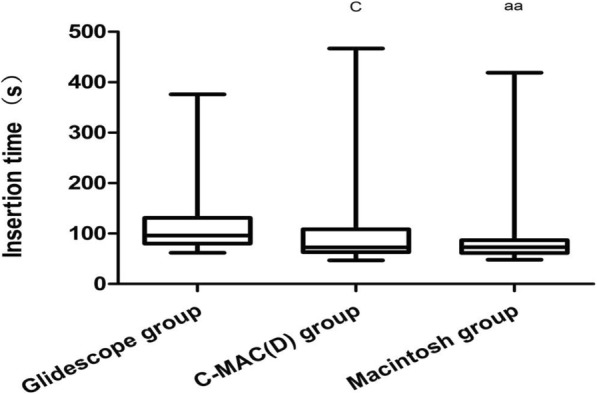
Results: Compared with the GlideScope, the Macintosh gave shorter times for DLT insertion (median: 96 (IQR: 51 [min-max: 62-376] s vs 73 (26 [48-419] s, p = 0.003); however, there was no difference between the Macintosh and C-MAC(D) (p = 0.610). The Macintosh had a significantly higher successful first attempt rate than did the GlideScope or C-MAC(D) (p = 0.001, p = 0.028, respectively). NRS of DLT delivery and insertion were significantly lower in the Macintosh than in the others (p < 0.001). However, the C/L degree in the Macintosh was significantly higher than in the others (p < 0.001). The incidences of oral bleeding, hoarseness, sore throat and dental trauma were low in all groups (p > 0.05). There were no significant differences in DLT misplacement, fiberoptic time or hemodynamic changes among the groups.
Conclusions: Compared with the Macintosh laryngoscope, the GlideScope® and C-MAC®(D) videolaryngoscopes may not be recommended as the first choice for routine DLT intubation in patients with predicted normal airways.
Trial registration: The study was prospectively registered at the Chinese Clinical Trial Registry (no. ChiCTR1900025718); principal investigator: Z.L.H.; date of registration: September 6, 2019.
Keywords: C-MAC®(D) videolaryngoscope; Double lumen tracheal tube; Endotracheal intubation; GlideScope® videolaryngoscope; Macintosh laryngoscope.
Conflict of interest statement
The authors have declared that no competing interest exists.
Figures



References
-
- Ahmed-Nusrath A. Focus on: ophthalmic anesthesia videolaryngoscopy. Curr Anaesth Crit Care. 2010;21:199–205. doi: 10.1016/j.cacc.2010.03.006. - DOI
-
- Serocki G, Neumann T, Scharf E, Dörges V, Cavus E. Indirect videolaryngoscopy with C-MAC D-blade and GlideScope: a randomized, controlled comparison in patients with suspected difficult airways. Minerva Anestesiol. 2013;79:121–129. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
