

Prevalence of surgical site infection and its associated factors after cesarean section in Ethiopia: systematic review and meta-analysis
- PMID: 32434486
- PMCID: PMC7238644
- DOI: 10.1186/s12884-020-03005-8
Prevalence of surgical site infection and its associated factors after cesarean section in Ethiopia: systematic review and meta-analysis
Abstract
Background: Surgical site infection (SSI) affects nearly one third of patients who have undergone a surgical procedure. It is a significant and substantial cause of surgical patient morbidity and mortality later with human and financial costs threat. There are fragmented and pocket studies which reported the prevalence of SSI among mothers who experienced for cesarean section and its risk factors. However, there is no any solid evidence established at the national level; which was also the interest of the authors to fill this gap. Therefore, this systematic review and meta-analysis aimed to estimate the pooled prevalence of SSI after cesarean section and its associated factors at national level.
Methods: Original articles were searched in PubMed, MEDLINE, EMBASE, CINAHL, Google Scholar, HINARI portal, and Cochrane Library. All observational studies defined outcome of variable "SSI as infection related to an operation procedure that occur at or near surgical incision within 30 days of operation or after one year if an implant is placed" were considered. Data were extracted using standard data extraction excel spread sheet checklists developed according to 2014 Joanna Briggs Institute Reviewers' Manual after the quality was assessed through Newcastle-Ottawa quality assessment scale. The I2 statistic was used to quantify heterogeneity across studies. Funnel plot asymmetry and Egger's tests were used to check for publication bias. A fixed effect model was used to estimate the pooled prevalence of SSI. Odds Ratio (OR) with 95% Confidence Interval (CI) was also considered to determine the association of identified variables with SSI. Statistical analysis was conducted using STATA version 14 software.
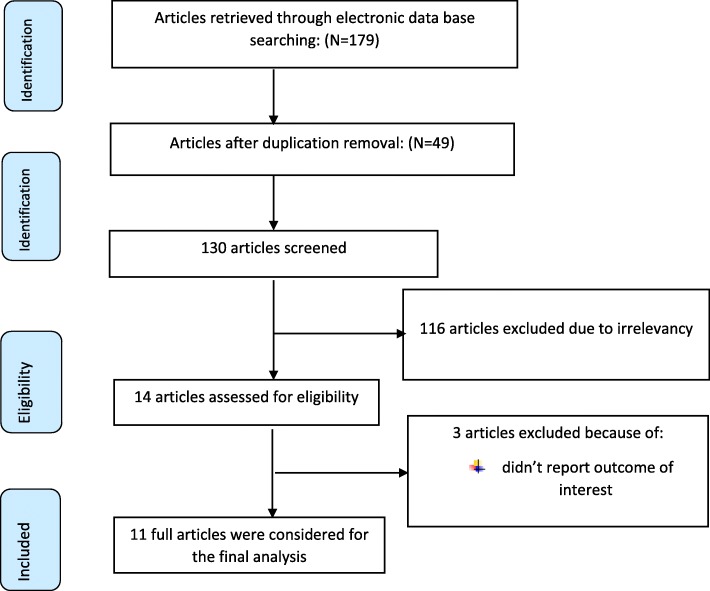
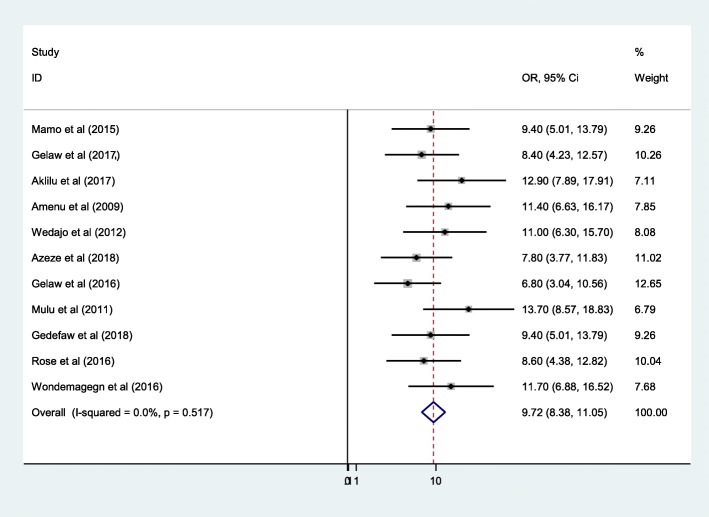
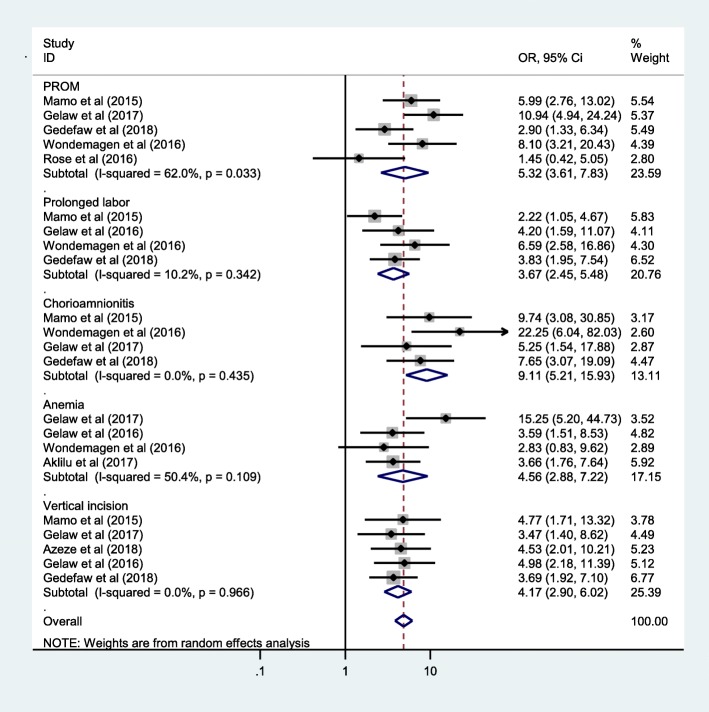
Result: From initial 179 identified articles, 11 were eligible for inclusion in the final systematic review and meta-analysis. Studies with a score of 6 and above were included for final analysis. All included studies were institutional based cross sectional. The pooled estimate of SSI after cesarean section in Ethiopia was 9.72% (95%CI: 8.38, 11.05). Premature rapture of membrane (PROM) > 12 h (OR = 5.32, 95%CI: 3.61, 7.83), duration of labor> 24 h (OR = 3.67, 95%CI: 2.45, 5.48), chorioamnionitis (OR = 9.11, 95%CI: 5.21, 15.93), anemia (OR = 4.56, 95%CI: 2.88, 7.22) and having vertical skin incision (OR = 4.17, 95%CI: 2.90, 6.02) had increased odds of developing SSI after cesarean section.
Conclusion: The prevalence of SSI after cesarean section in Ethiopia was high compared with the sphere standards of communicable disease control (CDC) guidelines for SSI after cesarean section. Therefore, Ministry of Health with its stake holders should give special emphasis on community and institution based programs in manner to prevent prolonged labor, PROM, chorioamnionitis and anemia which will also have synergistic impact on SSI after cesarean section. Moreover, there is also a call to health professionals not to use vertical incision as primary option of cesarean section to reduce the risk of developing surgical site infection among mothers.
Keywords: Cesarean section; Ethiopia; Prevalence; Surgical site infection.
Conflict of interest statement
The authors have declared that there are no competing interests.
Figures

Similar articles
-
Surgical site infection following cesarean section and its predictors in Ethiopia: A systematic review and meta-analysis.PLoS One. 2024 Mar 21;19(3):e0296767. doi: 10.1371/journal.pone.0296767. eCollection 2024. PLoS One. 2024. PMID: 38512861 Free PMC article.
-
Magnitude and Factors Associated With Post-Cesarean Surgical Site Infection at Hawassa University Teaching and Referral Hospital, Southern Ethiopia: A Cross-sectional Study.Ethiop J Health Sci. 2017 May;27(3):283-290. doi: 10.4314/ejhs.v27i3.10. Ethiop J Health Sci. 2017. PMID: 29217927 Free PMC article.
-
Surgical site infection and associated factors among women underwent cesarean delivery in Debretabor General Hospital, Northwest Ethiopia: hospital based cross sectional study.BMC Pregnancy Childbirth. 2019 Aug 29;19(1):317. doi: 10.1186/s12884-019-2442-0. BMC Pregnancy Childbirth. 2019. PMID: 31464598 Free PMC article.
-
Magnitude of postpartum hemorrhage and its associated factors in Ethiopia: a systematic review and meta-analysis.Reprod Health. 2022 Mar 9;19(1):63. doi: 10.1186/s12978-022-01360-7. Reprod Health. 2022. PMID: 35264188 Free PMC article.
-
Epidemiology of surgical site infections post-cesarean section in Africa: a comprehensive systematic review and meta-analysis.BMC Pregnancy Childbirth. 2025 Apr 22;25(1):465. doi: 10.1186/s12884-025-07526-y. BMC Pregnancy Childbirth. 2025. PMID: 40264037 Free PMC article.
Cited by
-
Surgical site infections post cesarean section and associated risk factors: a retrospective case-control study at a tertiary hospital in Kenya.Infect Prev Pract. 2023 Dec 13;6(1):100333. doi: 10.1016/j.infpip.2023.100333. eCollection 2024 Mar. Infect Prev Pract. 2023. PMID: 38222856 Free PMC article.
-
Effect of Low-Frequency Electric Pulse Technique Combined with Carboprost Methylate Suppositories on Recovery of Gastrointestinal Function and Postoperative Complications of Patients with Scarred Uterus Undergoing Secondary Cesarean Section.J Healthc Eng. 2021 Nov 24;2021:6143421. doi: 10.1155/2021/6143421. eCollection 2021. J Healthc Eng. 2021. PMID: 34868526 Free PMC article.
-
Determinants of Successful Vaginal Birth After Caesarean Section at Public Hospitals in Ambo Town, Oromia Region, Central Ethiopia: A Case-Control Study.Risk Manag Healthc Policy. 2021 Sep 29;14:4083-4091. doi: 10.2147/RMHP.S322380. eCollection 2021. Risk Manag Healthc Policy. 2021. PMID: 34616195 Free PMC article.
-
Vulnerabilities and reparative strategies during pregnancy, childbirth, and the postpartum period: moving from rhetoric to action.EClinicalMedicine. 2023 Dec 6;67:102264. doi: 10.1016/j.eclinm.2023.102264. eCollection 2024 Jan. EClinicalMedicine. 2023. PMID: 38314056 Free PMC article. Review.
-
Assessing Ethiopia's surgical capacity in light of global surgery 2030 initiatives: Is there progress in the past decade?Surg Open Sci. 2024 Mar 28;19:70-79. doi: 10.1016/j.sopen.2024.03.015. eCollection 2024 Jun. Surg Open Sci. 2024. PMID: 38595832 Free PMC article. Review.
References
-
- Leaper D, Edmiston C. World Health Organization: global guidelines for the prevention of surgical site infection. J Hosp Infect. 2017;95(2):135–136. - PubMed
-
- Steiner Holly L., Strand Eric A. Surgical-site infection in gynecologic surgery: pathophysiology and prevention. American Journal of Obstetrics and Gynecology. 2017;217(2):121–128. - PubMed
-
- Preas MA, O'Hara L, Thom K. 2017 HICPAC‐CDC guideline for prevention of surgical site infection: what the infection preventionist needs to know. Prevention Strategist. 2017.
-
- Leaper D.J., Edmiston C.E. World Health Organization: global guidelines for the prevention of surgical site infection. Journal of Hospital Infection. 2017;95(2):135–136. - PubMed
-
- Smith MA, Dahlen NR, Bruemmer A, Davis S, Heishman C. Clinical practice guideline surgical site infection prevention. Orthop Nurs. 2013;32(5):242–248. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
