

The clinical significance of the T2-FLAIR mismatch sign in grade II and III gliomas: a population-based study
- PMID: 32434559
- PMCID: PMC7238512
- DOI: 10.1186/s12885-020-06951-w
The clinical significance of the T2-FLAIR mismatch sign in grade II and III gliomas: a population-based study
Abstract
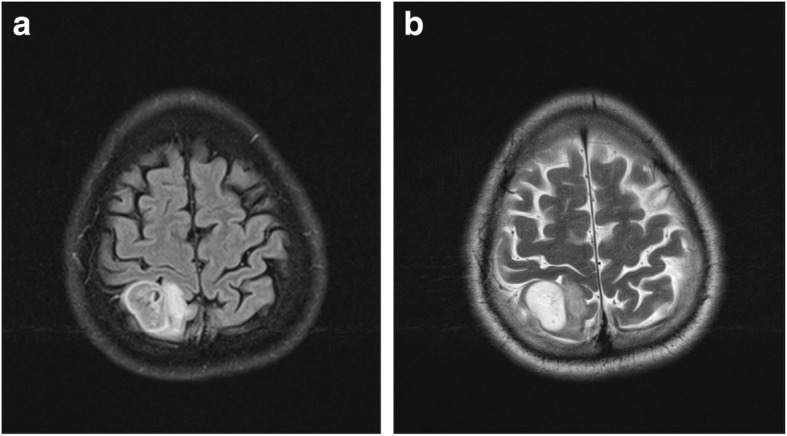
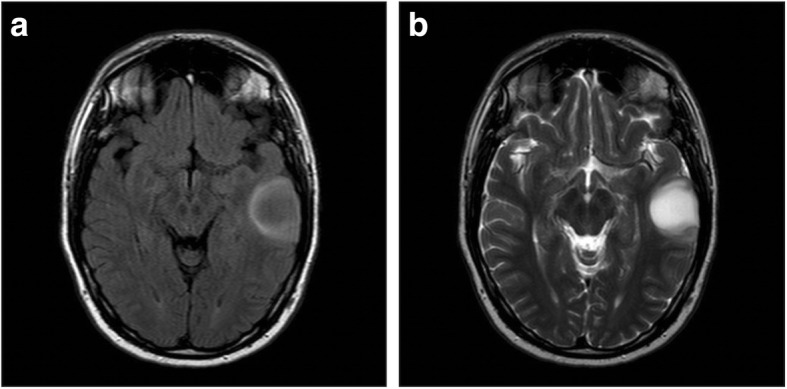
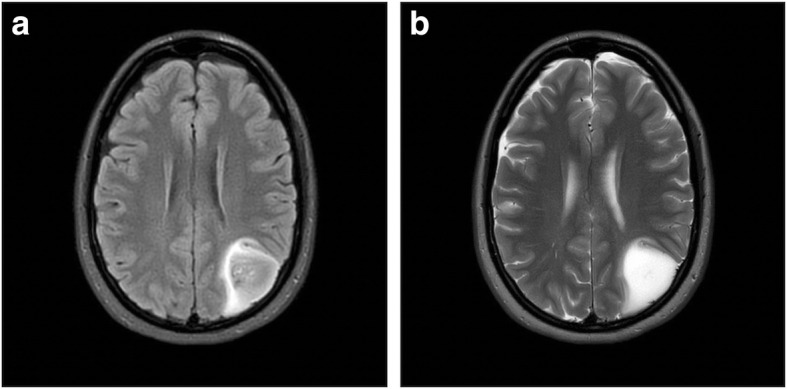
Background: The T2-FLAIR mismatch sign is an imaging finding highly suggestive of isocitrate dehydrogenase mutated (IDH-mut) 1p19q non-codeleted (non-codel) gliomas (astrocytomas). In previous studies, it has shown excellent specificity but limited sensitivity for IDH-mut astrocytomas. Whether the mismatch sign is a marker of a clinically relevant subtype of IDH-mut astrocytomas is unknown.
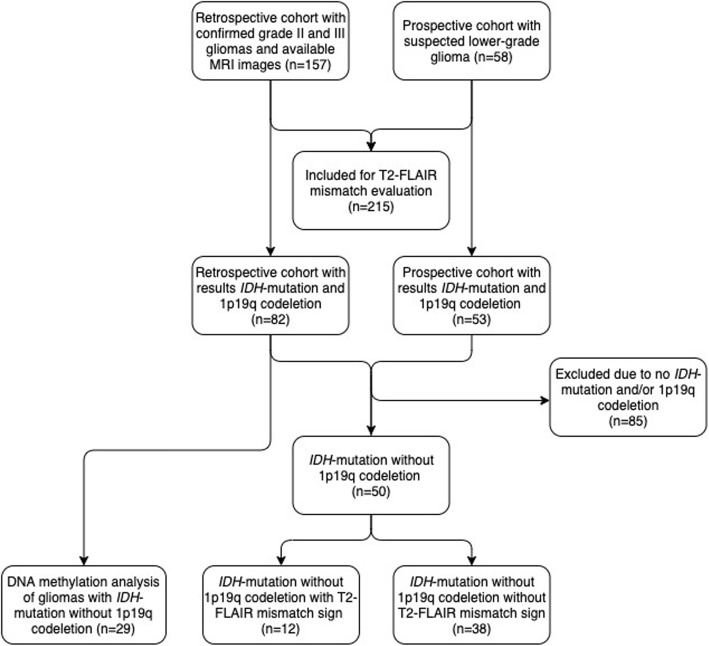
Methods: We included histopathologically verified supratentorial lower-grade gliomas (LGG) WHO grade II-III retrospectively during the period 2010-2016. In the period 2017-2018, patients with suspected LGG radiologically were prospectively included, and in this cohort other diagnoses than glioma could occur. Clinical, radiological and molecular data were collected. For clinical evaluation we included all patients with IDH-mut astrocytomas. In the 2010-2016 cohort DNA methylation analysis with Infinium MethylationEPIC BeadChip (Illumina) was performed for patients with an IDH-mut astrocytoma with available tissue. We aimed to examine the association of the T2-FLAIR mismatch sign with clinical factors and outcomes. Additionally, we evaluated the diagnostic reliability of the mismatch sign and its relation to methylation profiles.
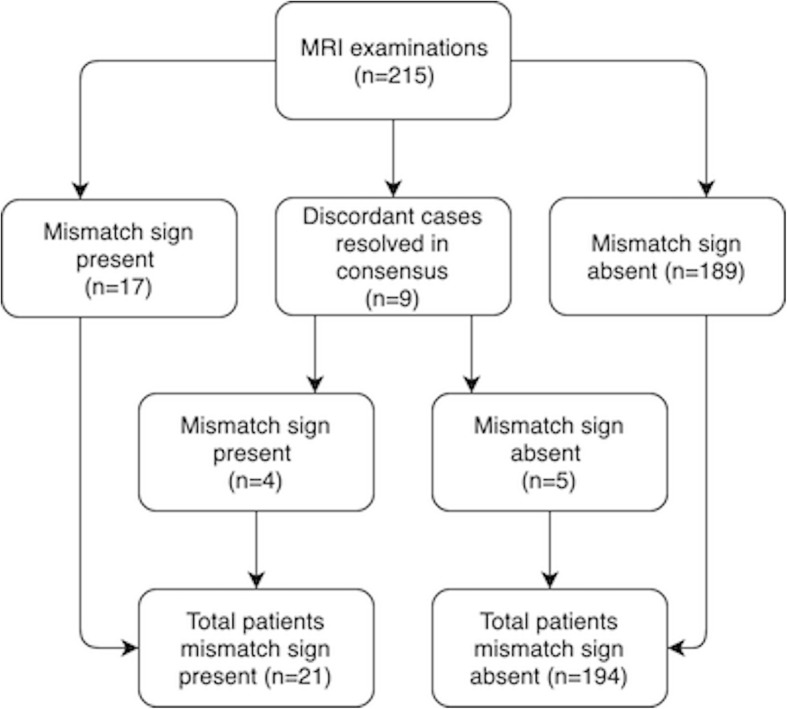
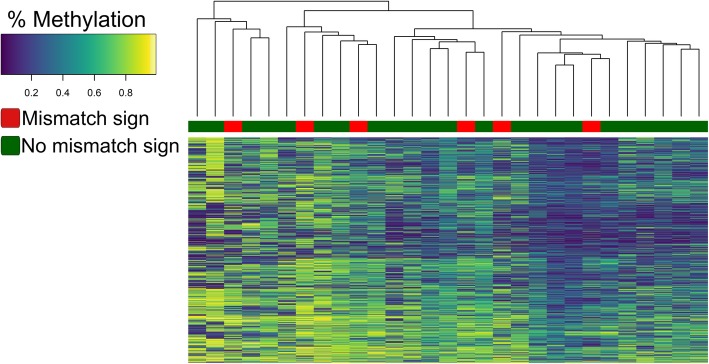
Results: Out of 215 patients with LGG, 135 had known IDH-mutation and 1p19q codeletion status. Fifty patients had an IDH-mut astrocytoma and 12 of these (24.0%) showed a mismatch sign. The sensitivity and specificity of the mismatch sign for IDH-mut detection were 26.4 and 97.6%, respectively. There were no differences between patients with an IDH-mut astrocytoma with or without mismatch sign when grouped according to T2-FLAIR mismatch sign with respect to baseline characteristics, clinical outcomes and methylation profiles. The overall interrater agreement between neuroradiologist and clinical neurosurgeons for the T2-FLAIR mismatch sign was significant when all 215 MRI examination assessed (κ = 0.77, p < 0.001, N = 215).
Conclusion: The T2-FLAIR mismatch sign in patients with an IDH-mut astrocytoma is not associated with clinical presentation or outcome. It seems unlikely that the IDH-mut astrocytomas with mismatch sign represent a specific subentity. Finally, we have validated that the T2-FLAIR mismatch sign is a reliable and specific marker of IDH-mut astrocytomas.
Keywords: Astrocytoma; Biomarkers; Decision making, prognosis; Oligodendroglioma.
Conflict of interest statement
All authors certify that they have no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria; educational grants; participation in speakers’ bureaus; membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements), or non-financial interest (such as personal or professional relationships, affiliations, knowledge or beliefs) in the subject matter or materials discussed in this manuscript.
Figures
References
-
- Louis DN, Perry A, Reifenberger G, von Deimling A, Figarella-Branger D, Cavenee WK, Ohgaki H, Wiestler OD, Kleihues P, Ellison DW. The 2016 World Health Organization classification of tumors of the central nervous system: a summary. Acta Neuropathol. 2016;131(6):803–820. - PubMed
-
- Etxaniz O, Carrato C, de Aguirre I, Queralt C, Munoz A, Ramirez JL, Rosell R, Villa S, Diaz R, Estival A, et al. IDH mutation status trumps the Pignatti risk score as a prognostic marker in low-grade gliomas. J Neuro-Oncol. 2017;135(2):273–284. - PubMed
-
- Sun H, Yin L, Li S, Han S, Song G, Liu N, Yan C. Prognostic significance of IDH mutation in adult low-grade gliomas: a meta-analysis. J Neuro-Oncol. 2013;113(2):277–284. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
