

Reversing 21 years of chronic paralysis via non-invasive spinal cord neuromodulation: a case study
- PMID: 32436278
- PMCID: PMC7261759
- DOI: 10.1002/acn3.51051
Reversing 21 years of chronic paralysis via non-invasive spinal cord neuromodulation: a case study
Abstract
Objective: The objective of the current study was to investigate if a non-invasive spinal cord neuromodulation modality could restore sensorimotor functions in a patient with chronic spinal cord injury (SCI).
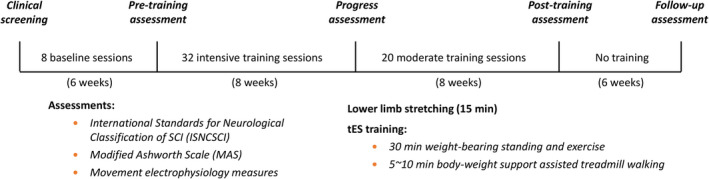
Methods: In this study, transcutaneous electrical stimulation (tES) to the spinal cord was utilized to restore sensorimotor functions in a chronic SCI patient who sustained a traumatic C7 cervical cord injury 21 years ago. At baseline, the patient had very limited volitional movement in her right leg, and her left leg was completely paralyzed. tES parameters were optimized in eight stimulation sessions before the treatment. The therapeutic stimulation involved biphasic tES, applied to T11 and L1 spinal levels during a 1-hour standing and walking training, 2-4 times per week for 16 weeks.
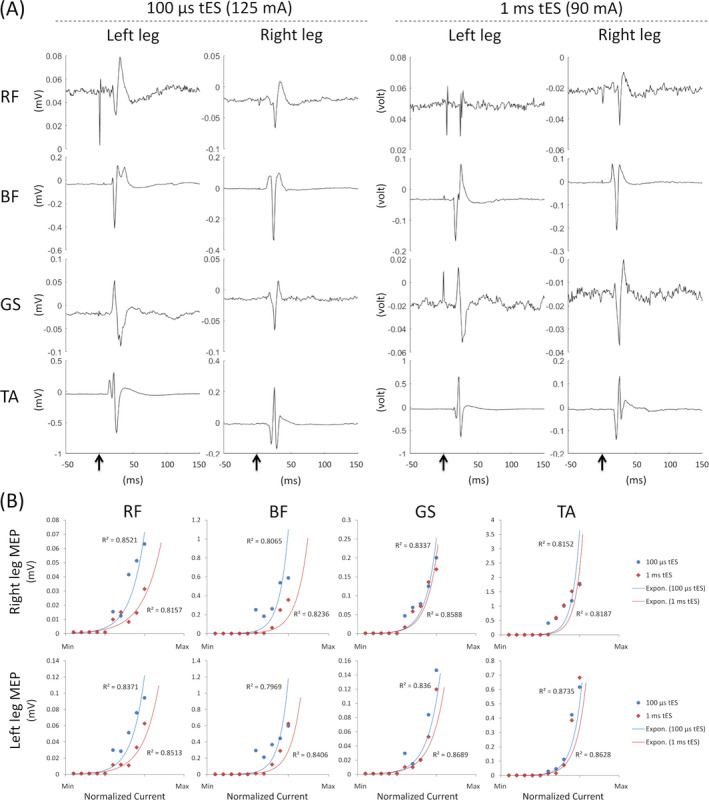
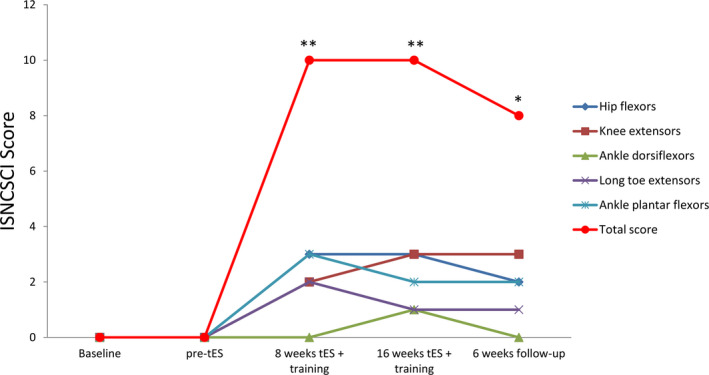
Results: Our pre-treatment tests indicated that a shorter burst duration (100 µsec) was more effective than a longer burst duration of tES in improving functional movements. After 32 training sessions with tES, the patient regained significant left-leg volitional movements (grade 0 to grade 10 according to the ISNCSCI scale). Right-leg motor scores also increased from 17 to 21. The tES treatment also improved her pinprick sensation (from 73 to 79). Upon completion of the treatment (52 sessions), the patient's standing ability noticeably improved. She could stabilize her knee to stand without any assistance. She could also squat while holding onto a walker.
Interpretation: These promising results demonstrate beneficial effects of non-invasive tES in regaining volitional control of plegic lower limbs in patients with chronic paralysis.
© 2020 The Authors. Annals of Clinical and Translational Neurology published by Wiley Periodicals LLC on behalf of American Neurological Association.
Conflict of interest statement
The authors declare no conflict of interest.
Figures


References
-
- Alam M, He J. Lower‐limb neuroprostheses: restoring walking after spinal cord injury In: Naik G. R. and Guo Y., eds. Emerging theory and practice in neuroprosthetics. pp. 153–180. Hershey, PA: IGI Global, 2014.
-
- Kumar R, Lim J, Mekary RA, et al. Traumatic spinal injury: global epidemiology and worldwide volume. World Neurosurg 2018;113:e345–e363. - PubMed
-
- Angeli CA, Boakye M, Morton RA, et al. Recovery of over‐ground walking after chronic motor complete spinal cord injury. N Engl J Med 2018;379(13):1244–1250. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
