

Increase in COVID-19 cases and case-fatality and case-recovery rates in Europe: A cross-temporal meta-analysis
- PMID: 32437052
- PMCID: PMC7280723
- DOI: 10.1002/jmv.26035
Increase in COVID-19 cases and case-fatality and case-recovery rates in Europe: A cross-temporal meta-analysis
Abstract
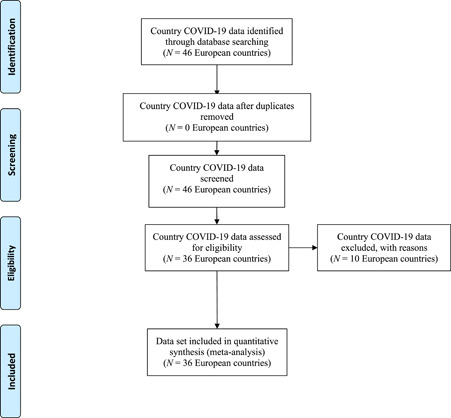
The new coronavirus (COVID-19) infection reported in China in December 2019 has become a pandemic in a few weeks, affecting the entire world. In this respect, it is crucial to determine the case-increase, case-fatality, and case-recovery rates to control COVID-19. In this study, the case-increase, case-fatality, and case-recovery rates of COVID-19 in 36 European countries were analyzed with the meta-analysis method using data released by the health organizations and WHO. The data were obtained from the website of health organizations of 36 European countries and the website of WHO until 11 May 2020. The analyses were carried out on 1 744 704 COVID-19-diagnosed cases in 36 European countries. The case-increase, case-fatality and case-recovery rates of COVID-19 were calculated using 95% confidence intervals (95% CI), single-arm meta-analysis, cross-temporal meta-analysis, and meta-regression random-effects model. The standardized case-increase rate of COVID-19 is 5% (95% CI [0.040, 0.063]) and the average case-increase rate in European countries has started to decline by around 3% (95% CI [0.047, 0.083]) weekly. The countries with the highest rate of case increase are Belgium, Sweden, Russia, the Netherlands and the United Kingdom. Although the case-fatality rate of COVID-19 patients was 4.5% as of May 11 (95% CI [0.037-0.055]), this rate is 6.3% (95% CI [0.047, 0.083]) in standardized time (6th week). The case-recovery rates of patients are 46% (95% CI [0.376-0.547]). This study presents important results regarding the COVID-19 pandemic in Europe. Although the rate of increase in new COVID-19 cases has dropped, there is not much decline in the case-fatality rates and no increase in case-recovery rates. The case-fatality rate of COVID-19 in Europe was estimated to be in the range of 4% to 4.5% and a minimum of 4 weeks (as of 11 May) is expected to have the figure below 1% in a country with an average case-increase rate. Monitoring case fatalities in Belgium, the Netherlands and Sweden, and treatment successes in Germany and Austria play a role of utmost importance.
Keywords: COVID-19; Europe; case-fatality rate; case-increase rate; case-recovery rate.
© 2020 Wiley Periodicals LLC.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
