

Pathology and Pathogenesis of SARS-CoV-2 Associated with Fatal Coronavirus Disease, United States
- PMID: 32437316
- PMCID: PMC7454055
- DOI: 10.3201/eid2609.202095
Pathology and Pathogenesis of SARS-CoV-2 Associated with Fatal Coronavirus Disease, United States
Abstract
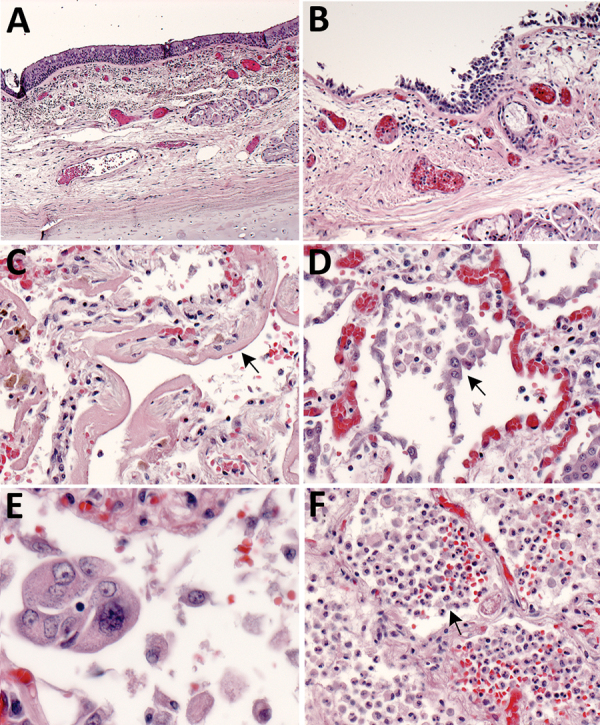
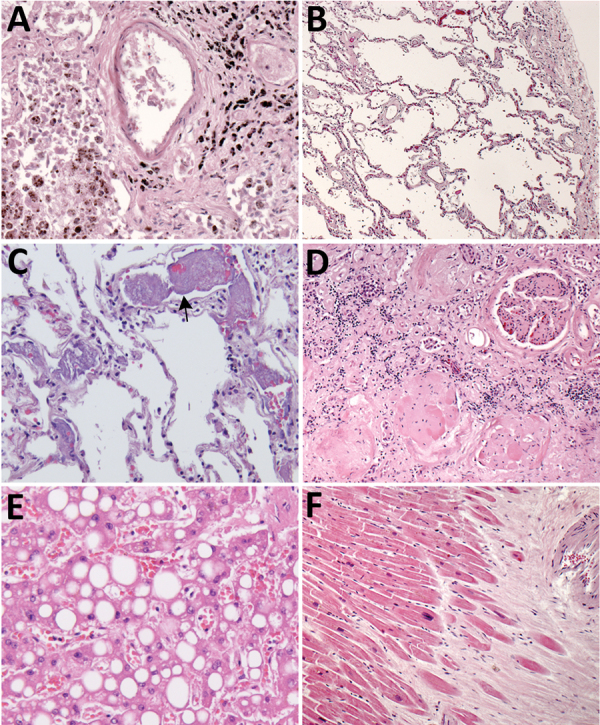
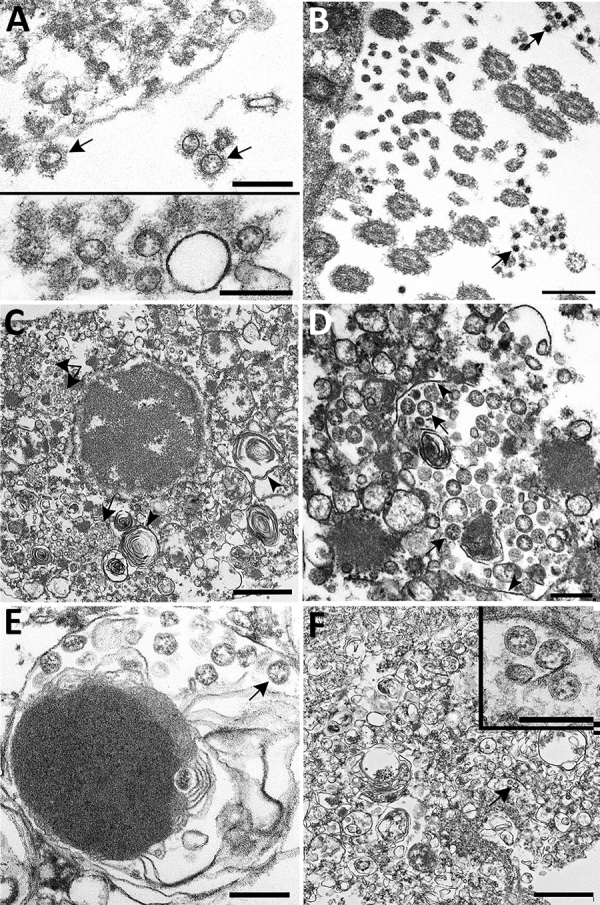
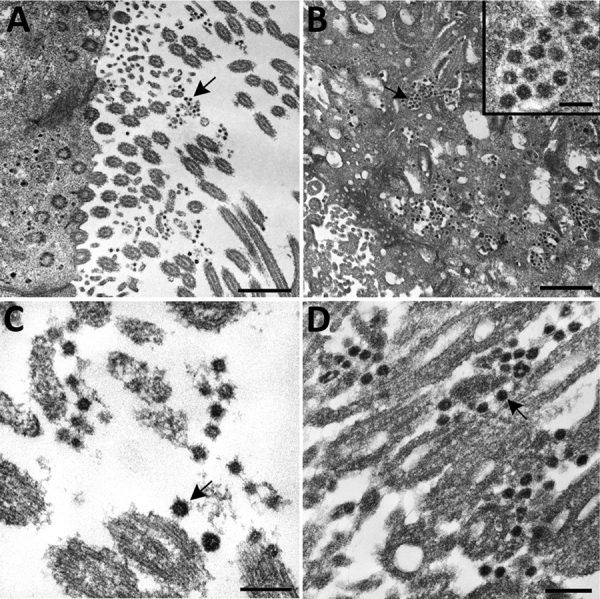
An ongoing pandemic of coronavirus disease (COVID-19) is caused by infection with severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2). Characterization of the histopathology and cellular localization of SARS-CoV-2 in the tissues of patients with fatal COVID-19 is critical to further understand its pathogenesis and transmission and for public health prevention measures. We report clinicopathologic, immunohistochemical, and electron microscopic findings in tissues from 8 fatal laboratory-confirmed cases of SARS-CoV-2 infection in the United States. All cases except 1 were in residents of long-term care facilities. In these patients, SARS-CoV-2 infected epithelium of the upper and lower airways with diffuse alveolar damage as the predominant pulmonary pathology. SARS-CoV-2 was detectable by immunohistochemistry and electron microscopy in conducting airways, pneumocytes, alveolar macrophages, and a hilar lymph node but was not identified in other extrapulmonary tissues. Respiratory viral co-infections were identified in 3 cases; 3 cases had evidence of bacterial co-infection.
Keywords: 2019 novel coronavirus disease; COVID-19; SARS-CoV-2; coronavirus; coronavirus disease; diffuse alveolar damage; electron microscopy; histopathology; immunohistochemistry; pathology; respiratory infections; severe acute respiratory syndrome coronavirus 2; viruses; zoonoses.
Figures

References
-
- World Health Organization. Coronavirus disease (COVID-19) pandemic. 2020. May 4 [cited 2020 May 5]. https://www.who.int/emergencies/diseases/novel-coronavirus-2019
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous
