

Association of Ketamine With Psychiatric Symptoms and Implications for Its Therapeutic Use and for Understanding Schizophrenia: A Systematic Review and Meta-analysis
- PMID: 32437573
- PMCID: PMC7243091
- DOI: 10.1001/jamanetworkopen.2020.4693
Association of Ketamine With Psychiatric Symptoms and Implications for Its Therapeutic Use and for Understanding Schizophrenia: A Systematic Review and Meta-analysis
Abstract
Importance: Ketamine hydrochloride is increasingly used to treat depression and other psychiatric disorders but can induce schizophrenia-like or psychotomimetic symptoms. Despite this risk, the consistency and magnitude of symptoms induced by ketamine or what factors are associated with these symptoms remain unknown.
Objective: To conduct a meta-analysis of the psychopathological outcomes associated with ketamine in healthy volunteers and patients with schizophrenia and the experimental factors associated with these outcomes.
Data sources: MEDLINE, Embase, and PsychINFO databases were searched for within-participant, placebo-controlled studies reporting symptoms using the Brief Psychiatric Rating Scale (BPRS) or the Positive and Negative Syndrome Scale (PANSS) in response to an acute ketamine challenge in healthy participants or patients with schizophrenia.
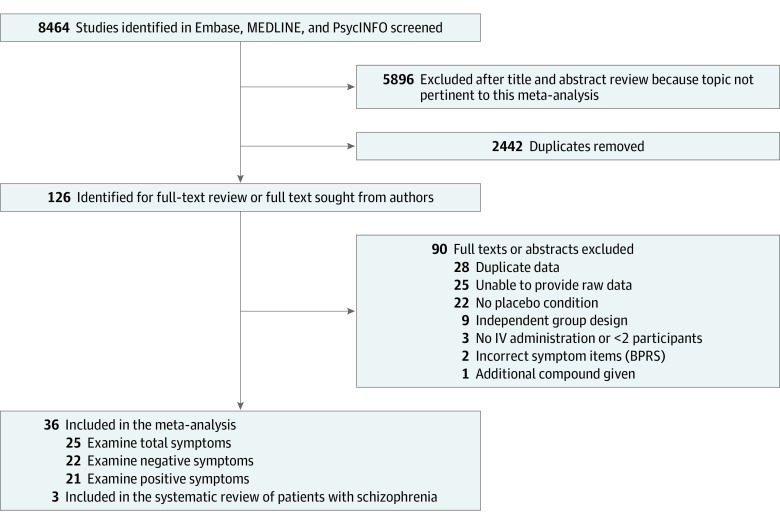
Study selection: Of 8464 citations retrieved, 36 studies involving healthy participants were included. Inclusion criteria were studies (1) including healthy participants; (2) reporting symptoms occurring in response to acute administration of subanesthetic doses of ketamine (racemic ketamine, s-ketamine, r-ketamine) intravenously; (3) containing a placebo condition with a within-subject, crossover design; (4) measuring total positive or negative symptoms using BPRS or PANSS; and (5) providing data allowing the estimation of the mean difference and deviation between the ketamine and placebo condition.
Data extraction and synthesis: Two independent investigators extracted study-level data for a random-effects meta-analysis. Total, positive, and negative BPRS and PANSS scores were extracted. Subgroup analyses were conducted examining the effects of blinding status, ketamine preparation, infusion method, and time between ketamine and placebo conditions. The Meta-analysis of Observational Studies in Epidemiology (MOOSE) and Preferred Reporting Items for Systematic Reviews and Meta-analyses (PRISMA) guidelines were followed.
Main outcomes and measures: Standardized mean differences (SMDs) were used as effect sizes for individual studies. Standardized mean differences between ketamine and placebo conditions were calculated for total, positive, and negative BPRS and PANSS scores.
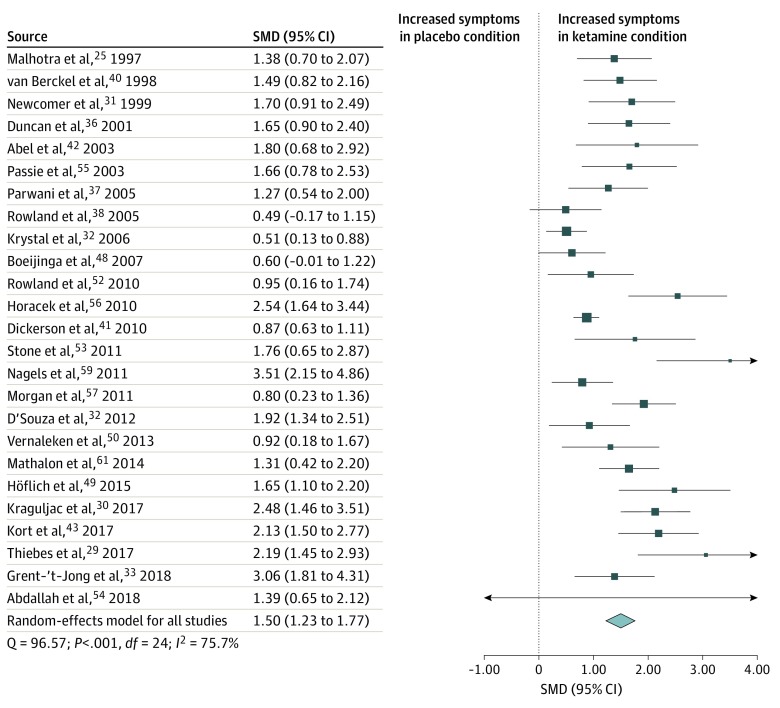
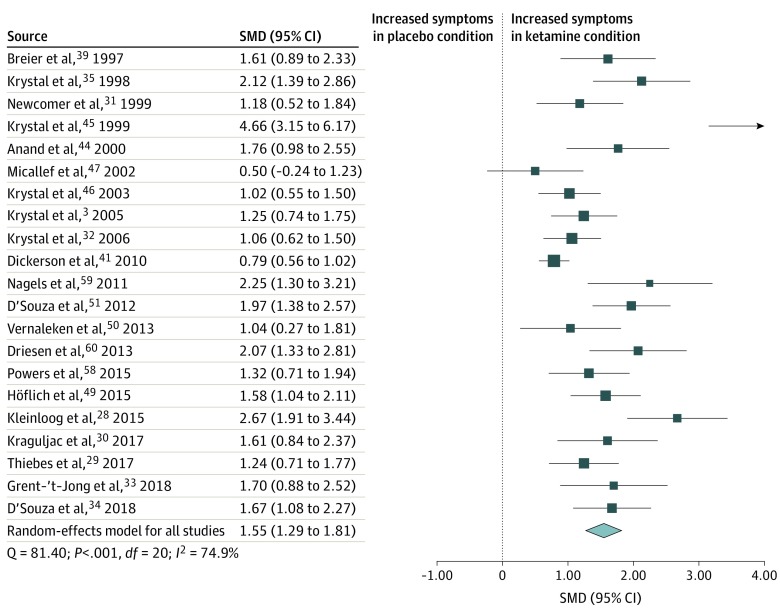
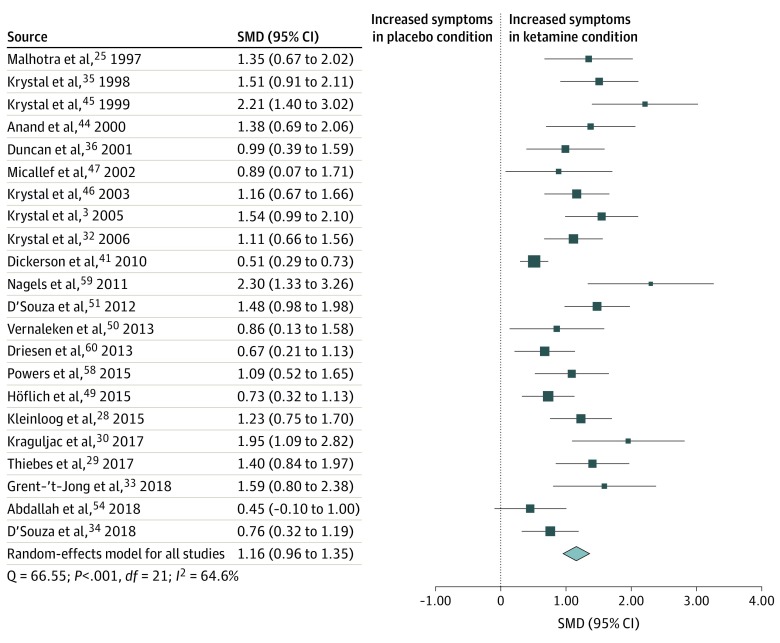
Results: The overall sample included 725 healthy volunteers (mean [SD] age, 28.3 [3.6] years; 533 [73.6%] male) exposed to the ketamine and placebo conditions. Racemic ketamine or S-ketamine was associated with a statistically significant increase in transient psychopathology in healthy participants for total (SMD = 1.50 [95% CI, 1.23-1.77]; P < .001), positive (SMD = 1.55 [95% CI, 1.29-1.81]; P < .001), and negative (SMD = 1.16 [95% CI, 0.96-1.35]; P < .001) symptom ratings relative to the placebo condition. The effect size for this association was significantly greater for positive than negative symptoms of psychosis (estimate, 0.36 [95% CI, 0.12-0.61]; P = .004). There was significant inconsistency in outcomes between studies (I2 range, 77%-83%). Bolus followed by constant infusion increased ketamine's association with positive symptoms relative to infusion alone (effect size, 1.63 [95% CI, 1.36-1.90] vs 0.84 [95% CI, 0.35-1.33]; P = .006). Single-day study design increased ketamine's ability to generate total symptoms (effect size, 2.29 [95% CI, 1.69-2.89] vs 1.39 [95% CI, 1.12-1.66]; P = .007), but age and sex did not moderate outcomes. Insufficient studies were available for meta-analysis of studies in schizophrenia. Of these studies, 2 found a statistically significant increase in symptoms with ketamine administration in total and positive symptoms. Only 1 study found an increase in negative symptom severity with ketamine.
Conclusions and relevance: This study found that acute ketamine administration was associated with schizophrenia-like or psychotomimetic symptoms with large effect sizes, but there was a greater increase in positive than negative symptoms and when a bolus was used. These findings suggest that bolus doses should be avoided in the therapeutic use of ketamine to minimize the risk of inducing transient positive (psychotic) symptoms.
Conflict of interest statement
Figures
References
-
- Stevenson C. Ketamine: a review. Updat Anaesth. 2005;20(20):25-29.
-
- Krystal JH, Perry EB Jr, Gueorguieva R, et al. Comparative and interactive human psychopharmacologic effects of ketamine and amphetamine: implications for glutamatergic and dopaminergic model psychoses and cognitive function. Arch Gen Psychiatry. 2005;62(9):985-994. doi: 10.1001/archpsyc.62.9.985 - DOI - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
