

First-line pembrolizumab and trastuzumab in HER2-positive oesophageal, gastric, or gastro-oesophageal junction cancer: an open-label, single-arm, phase 2 trial
- PMID: 32437664
- PMCID: PMC8229851
- DOI: 10.1016/S1470-2045(20)30169-8
First-line pembrolizumab and trastuzumab in HER2-positive oesophageal, gastric, or gastro-oesophageal junction cancer: an open-label, single-arm, phase 2 trial
Abstract
Background: Addition of trastuzumab to first-line chemotherapy improves overall survival in patients with HER2-positive metastatic gastric cancer. We assessed the safety and activity of pembrolizumab in combination with trastuzumab and chemotherapy in first-line HER2-positive metastatic oesophagogastric (gastric, oesophageal, or gastroesophageal junction) cancer.
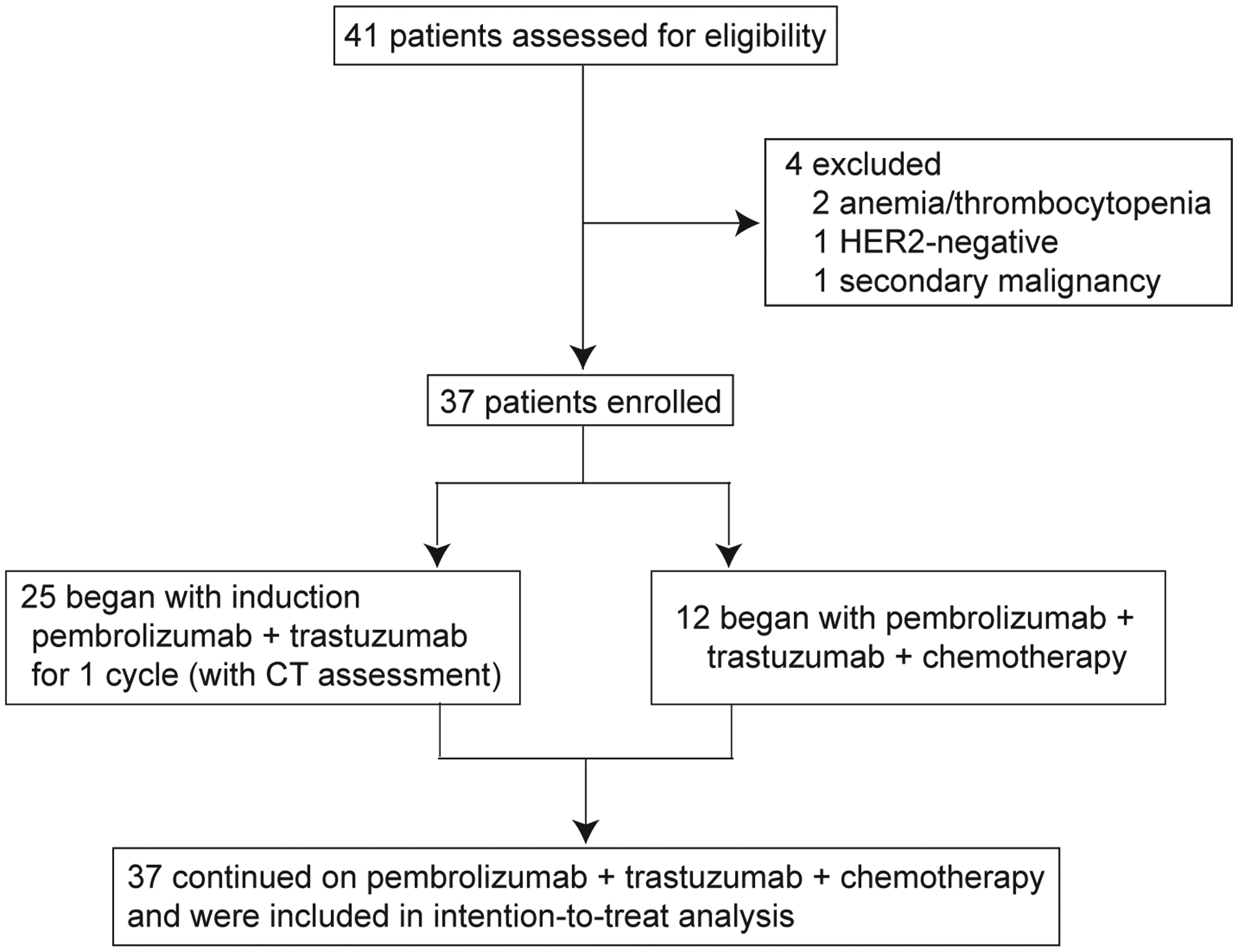
Methods: This study was an investigator-initiated, open-label, non-randomised, single-arm, single centre, phase 2 trial in patients aged 18 years or older with HER2-positive metastatic oesophagogastric cancer. Eligible patients had measurable or evaluable non-measurable disease, Eastern Cooperative Oncology Group performance status of 0, 1, or 2, and left ventricular ejection fraction of at least 53%. Patients were eligible to receive an initial induction cycle of 200 mg flat dose of intravenous pembrolizumab and 8 mg/kg loading dose of intravenous trastuzumab. For subsequent cycles, patients received 130 mg/m2 of intravenous oxaliplatin or 80 mg/m2 of cisplatin on day 1, 850 mg/m2 of oral capecitabine twice a day for 2 weeks followed by 1 week off (or intravenous 5-fluorouracil, 800 mg/m2 per day on days 1-5), and a 200 mg flat dose of intravenous pembrolizumab, and 6 mg/kg of trastuzumab, administered on day 1 of each 3-week cycle. The primary endpoint was 6-month progression-free survival, defined as the proportion of patients alive and free of progression at 6 months, assessed in patients who received at least one dose of trastuzumab and pembrolizumab. The regimen would be considered worthy of further investigation if 26 or more of 37 patients were progression-free at 6 months. This trial is registered with ClinicalTrials.gov, NCT02954536, and is ongoing, but closed to enrolment.
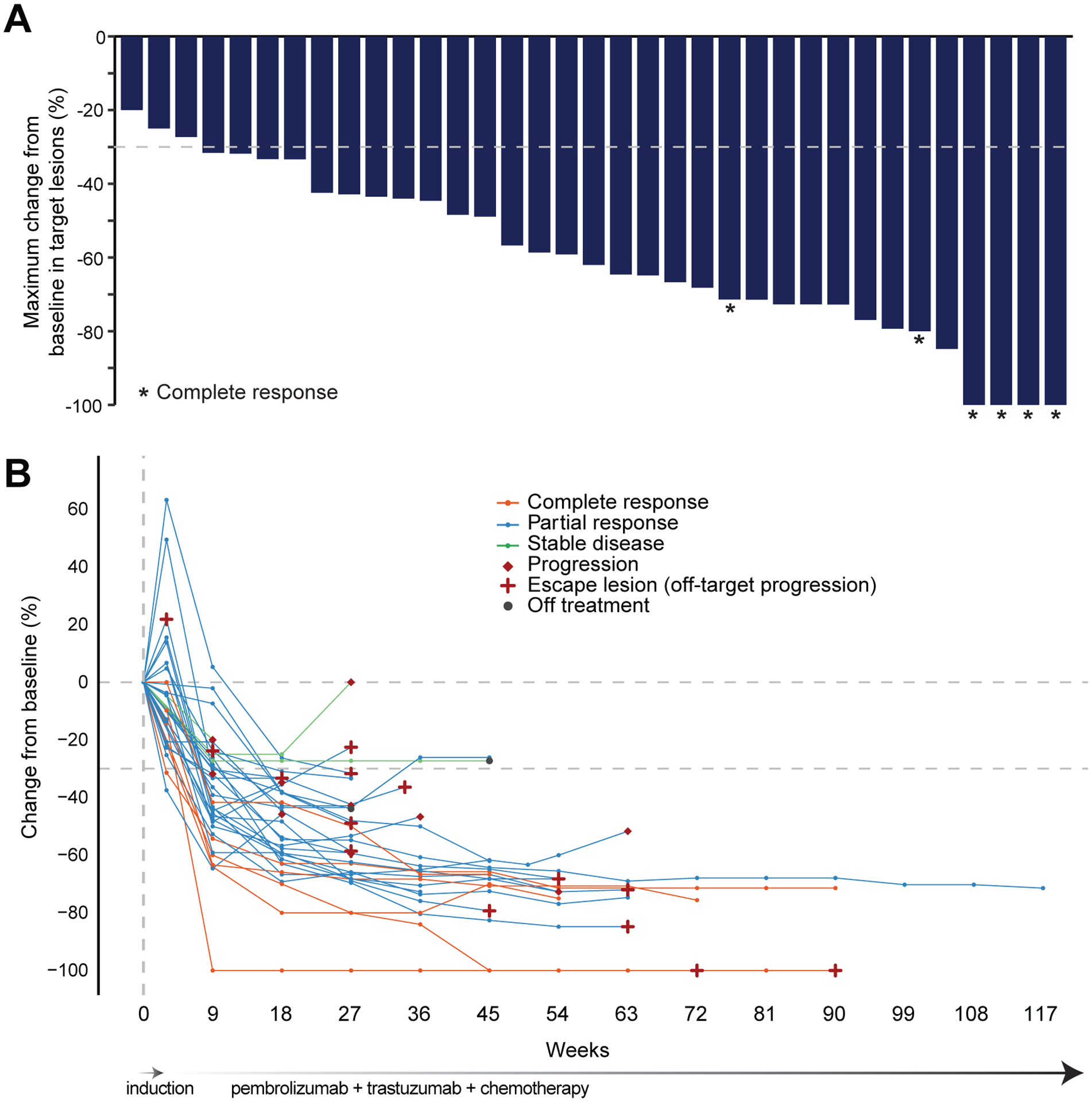
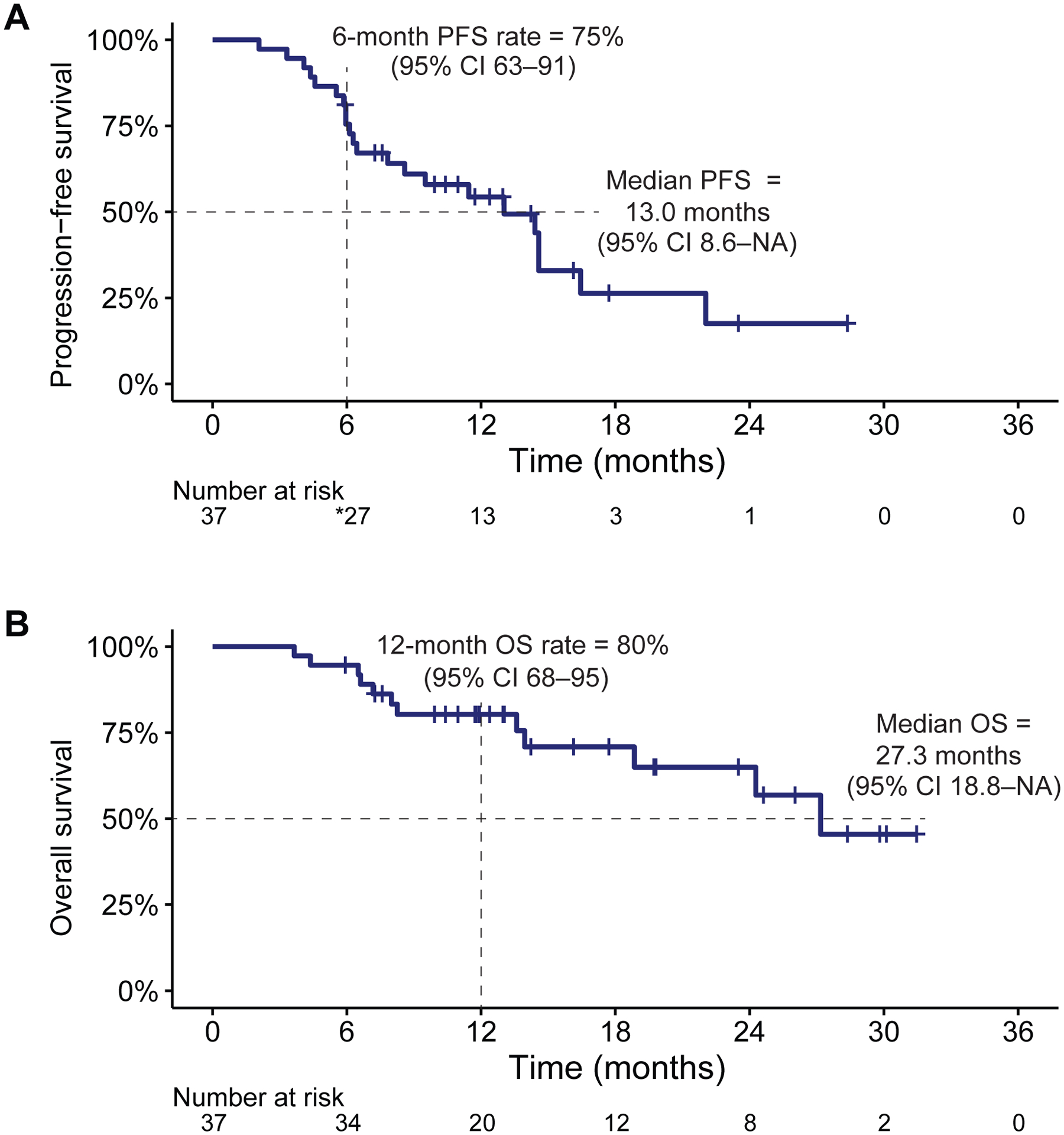
Findings: Between Nov 11, 2016, and Jan 23, 2019, 37 patients were enrolled. At the time of data cutoff on Aug 6, 2019, median follow-up among survivors was 13·0 months (IQR 11·7-23·5). The primary endpoint was achieved; 26 (70%; 95% CI 54-83) of 37 patients were progression-free at 6 months. The most common treatment-related adverse event of any grade was neuropathy, which was reported in 36 (97%) of 37 patients. The most common grade 3 or 4 adverse events were lymphocytopenia (seven [19%] patients with grade 3 and two [5%] with grade 4), grade 3 decreased electrolytes (six [16%] patients), and grade 3 anaemia (four [11%] patients). Serious adverse events occurred in two patients patients (both grade 3 nephritis leading to treatment discontinuation). Four patients discontinued pembrolizumab because of immune-related adverse events. There were no treatment-related deaths.
Interpretation: Pembrolizumab can be safely combined with trastuzumab and chemotherapy and has promising activity in HER2-positive metastatic oesophagogastric cancer. A randomised phase 3 clinical trial assessing the efficacy and safety of pembrolizumab versus placebo in combination with trastuzumab and chemotherapy in first-line HER2-positive metastatic oesophagogastric cancer is underway.
Funding: Merck & Co.
Copyright © 2020 Elsevier Ltd. All rights reserved.
Figures
Comment in
-
Immune checkpoint inhibitor plus anti-HER2 therapy: a new standard for HER2-positive oesophagogastric cancer?Lancet Oncol. 2020 Jun;21(6):741-743. doi: 10.1016/S1470-2045(20)30208-4. Epub 2020 May 18. Lancet Oncol. 2020. PMID: 32437663 No abstract available.
References
-
- Bray F, Ferlay J, Soerjomataram I, Siegel RL, Torre LA, Jemal A. Global cancer statistics 2018: GLOBOCAN estimates of incidence and mortality worldwide for 36 cancers in 185 countries. CA Cancer J Clin 2018; 68: 394–424. - PubMed
-
- Bartel M, Brahmbhatt B, Bhurwal A. Incidence of gastroesophageal junction cancer continues to rise: Analysis of Surveillance, Epidemiology, and End Results (SEER) database. J Clin Oncol 2019; 37: 40–40.
Publication types
MeSH terms
Substances
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
