

SARS-CoV-2 infection of the liver directly contributes to hepatic impairment in patients with COVID-19
- PMID: 32437830
- PMCID: PMC7211738
- DOI: 10.1016/j.jhep.2020.05.002
SARS-CoV-2 infection of the liver directly contributes to hepatic impairment in patients with COVID-19
Abstract
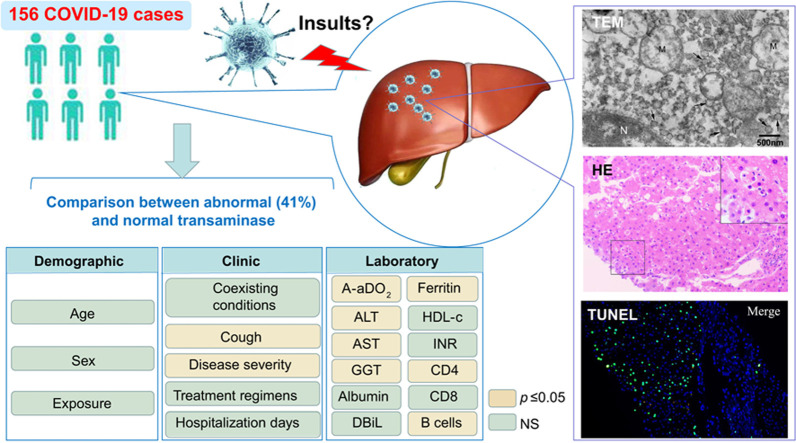
Background & aims: Liver enzyme abnormalities are common in patients with coronavirus disease 2019 (COVID-19). Whether or not severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) infection can lead to liver damage per se remains unknown. Herein, we reported the clinical characteristics and liver pathological manifestations of COVID-19 patients with liver enzyme abnormalities.
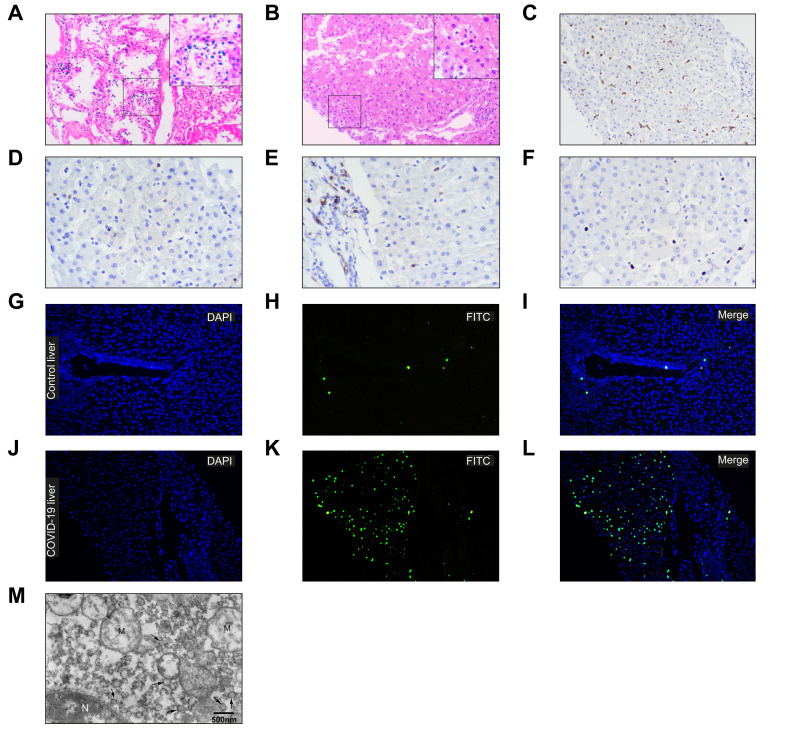
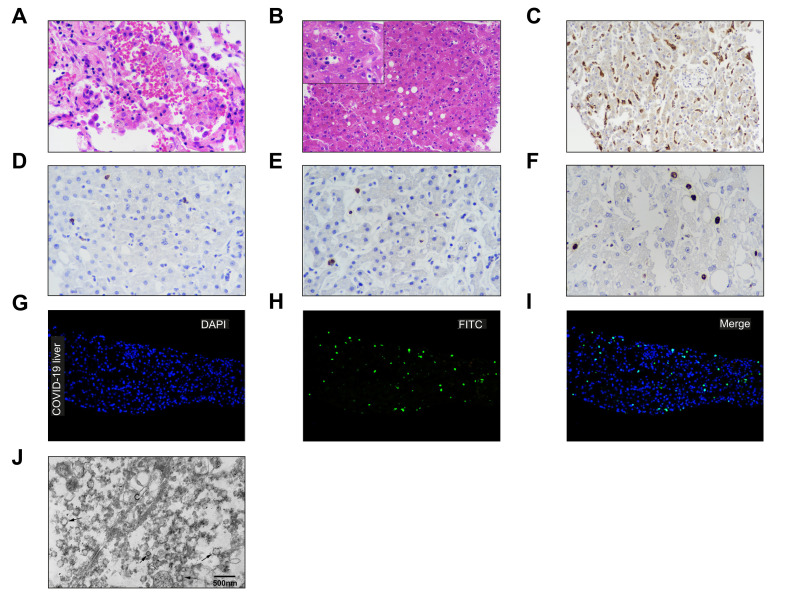
Methods: We analyzed 156 patients diagnosed with COVID-19 from 2 designated centers in China and compared clinical features between patients with or without elevated aminotransferases. Postmortem liver biopsies were obtained from 2 cases who had elevated aminotransferases. We investigated the patterns of liver impairment by electron microscopy, immunohistochemistry, TUNEL assay and pathological studies.
Results: Sixty-four out of 156 (41.0%) patients with COVID-19 had elevated aminotransferases. The median levels of alanine aminotransferase were 50 U/L vs. 19 U/L, respectively, aspartate aminotransferase were 45.5 U/L vs. 24 U/L, respectively in abnormal and normal aminotransferase groups. Liver enzyme abnormalities were associated with disease severity, as well as a series of laboratory tests including higher alveolar-arterial oxygen partial pressure difference, higher gamma-glutamyltransferase, lower albumin, decreased CD4+ T cells and B lymphocytes. Ultrastructural examination identified typical coronavirus particles, characterized by spike structures, in the cytoplasm of hepatocytes in 2 COVID-19 cases. SARS-CoV-2-infected hepatocytes displayed conspicuous mitochondrial swelling, endoplasmic reticulum dilatation and glycogen granule decrease. Histologically, massive hepatic apoptosis and some binuclear hepatocytes were observed. Taken together, both ultrastructural and histological evidence indicated a typical lesion of viral infection. Immunohistochemical results showed scarce CD4+ and CD8+ lymphocytes. No obvious eosinophil infiltration, cholestasis, fibrin deposition, granuloma, massive central necrosis, or interface hepatitis were observed.
Conclusions: SARS-CoV-2 infection in the liver directly contributes to hepatic impairment in patients with COVID-19. Hence, a surveillance of viral clearance in liver and long-term outcome of COVID-19 is required.
Lay summary: Liver enzyme abnormalities are common in patients with coronavirus disease 2019 (COVID-19). We reported the clinical characteristics and liver pathological manifestations of COVID-19 patients with elevated liver enzymes. Our findings suggested that SARS-CoV-2 infection of the liver is a crucial factor contributing to hepatic impairment in patients with COVID-19.
Keywords: COVID-19; Cytopathy; Liver enzyme abnormality; SARS-CoV-2 infection; Transaminase.
© 2020 European Association for the Study of the Liver. Published by Elsevier B.V. All rights reserved.
Conflict of interest statement
The authors declare no conflicts of interest that pertain to this work. Please refer to the accompanying ICMJE disclosure forms for further details.
Figures
Comment in
-
SARS-CoV-2 related liver impairment - perception may not be the reality.J Hepatol. 2020 Oct;73(4):991-992. doi: 10.1016/j.jhep.2020.05.025. Epub 2020 May 23. J Hepatol. 2020. PMID: 32454042 Free PMC article. No abstract available.
-
Single cell RNA sequencing analysis did not predict hepatocyte infection by SARS-CoV-2.J Hepatol. 2020 Oct;73(4):993-995. doi: 10.1016/j.jhep.2020.05.030. Epub 2020 May 28. J Hepatol. 2020. PMID: 32473193 Free PMC article. No abstract available.
-
SARS-CoV-2: Is the liver merely a bystander to severe disease?J Hepatol. 2020 Oct;73(4):995-996. doi: 10.1016/j.jhep.2020.05.035. Epub 2020 Jun 2. J Hepatol. 2020. PMID: 32502510 Free PMC article. No abstract available.
References
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
