

Tryptophan Metabolism, Inflammation, and Oxidative Stress in Patients with Neurovascular Disease
- PMID: 32438592
- PMCID: PMC7281607
- DOI: 10.3390/metabo10050208
Tryptophan Metabolism, Inflammation, and Oxidative Stress in Patients with Neurovascular Disease
Abstract
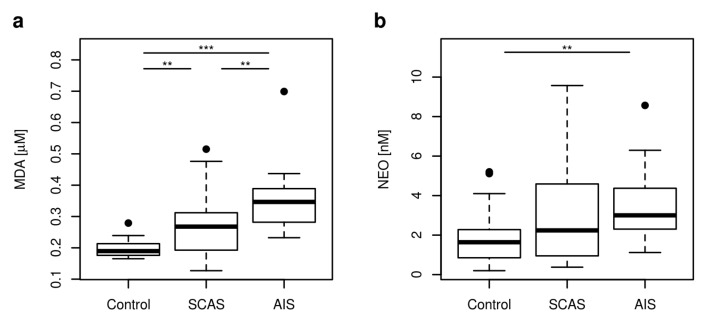
Atherosclerosis is a leading cause of major vascular events, myocardial infarction, and ischemic stroke. Tryptophan (TRP) catabolism was recognized as an important player in inflammation and immune response having together with oxidative stress (OS) significant effects on each phase of atherosclerosis. The aim of the study is to analyze the relationship of plasma levels of TRP metabolites, inflammation, and OS in patients with neurovascular diseases (acute ischemic stroke (AIS), significant carotid artery stenosis (SCAS)) and in healthy controls. Blood samples were collected from 43 patients (25 with SCAS, 18 with AIS) and from 25 healthy controls. The concentrations of twelve TRP metabolites, riboflavin, neopterin (NEO, marker of inflammation), and malondialdehyde (MDA, marker of OS) were measured by liquid chromatography-tandem mass spectrometry (LC-MS/MS). Concentrations of seven TRP metabolites (TRP, kynurenine (KYN), 3-hydroxykynurenine (3-HK), 3-hydroxyanthranilic acid (3-HAA), anthranilic acid (AA), melatonin (MEL), tryptamine (TA)), NEO, and MDA were significantly different in the studied groups. Significantly lower concentrations of TRP, KYN, 3-HAA, MEL, TA, and higher MDA concentrations were found in AIS compared to SCAS patients. MDA concentration was higher in both AIS and SCAS group (p < 0.001, p = 0.004, respectively) compared to controls, NEO concentration was enhanced (p < 0.003) in AIS. MDA did not directly correlate with TRP metabolites in the study groups, except for 1) a negative correlation with kynurenine acid and 2) the activity of kynurenine aminotransferase in AIS patients (r = -0.552, p = 0.018; r = -0.504, p = 0.033, respectively). In summary, TRP metabolism is clearly more deregulated in AIS compared to SCAS patients; the effect of TRP metabolites on OS should be further elucidated.
Keywords: acute ischemic stroke; atherosclerosis; carotid artery stenosis; inflammation; oxidative stress; tryptophan metabolism.
Conflict of interest statement
The authors declare no conflict of interest.
Figures







References
Grants and funding
- NV18-08-00149/Czech health research council
- CZ.02.1.01/0.0/0.0/16_025/0007428, OP RDE/European Regional Development Fund and the state budget of the Czech Republic
- 00023736/Project of the Ministry of Health, Czech Republic
- 1011/Long-term organization development plan, Faculty of Military Health Sciences, Hradec Kralove
LinkOut - more resources
Full Text Sources
Other Literature Sources
