

Physiological Stratification of Patients With Angina Due to Coronary Microvascular Dysfunction
- PMID: 32439003
- PMCID: PMC7242900
- DOI: 10.1016/j.jacc.2020.03.051
Physiological Stratification of Patients With Angina Due to Coronary Microvascular Dysfunction
Abstract
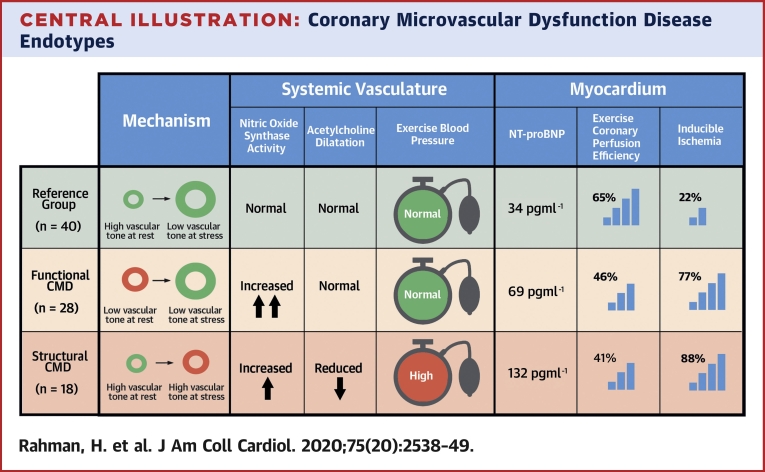
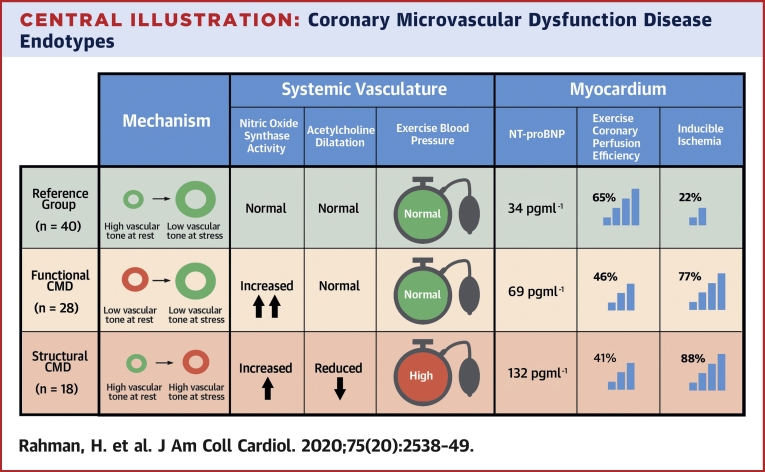
Background: Coronary microvascular dysfunction (CMD) is defined by diminished flow reserve. Functional and structural CMD endotypes have recently been described, with normal and elevated minimal microvascular resistance, respectively.
Objectives: This study determined the mechanism of altered resting and maximal flow in CMD endotypes.
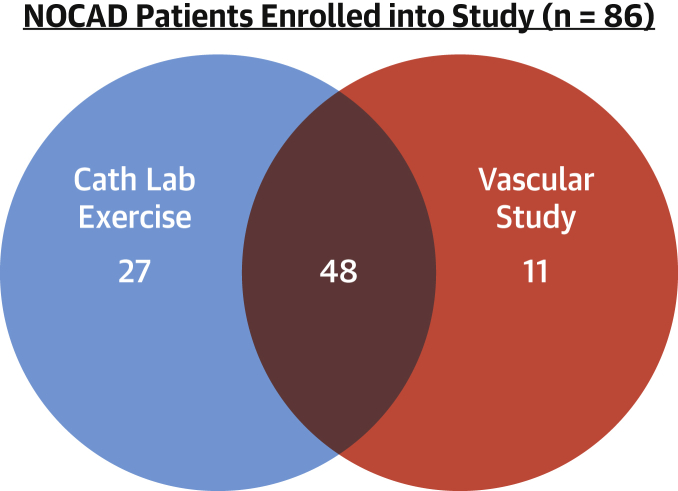
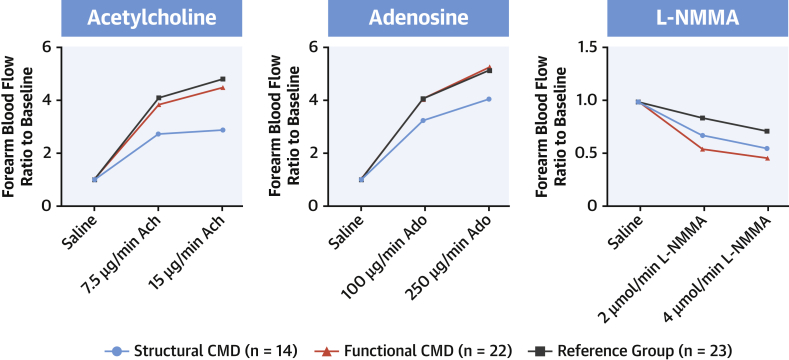
Methods: A total of 86 patients with angina but no obstructive coronary disease underwent coronary pressure and flow measurement during rest, exercise, and adenosine-mediated hyperemia and were classified as the reference group or as patients with CMD by a coronary flow reserve threshold of 2.5; functional or structural endotypes were distinguished by a hyperemic microvascular resistance threshold of 2.5 mm Hg/cm/s. Endothelial function was assessed by forearm blood flow (FBF) response to acetylcholine, and nitric oxide synthase (NOS) activity was defined as the inverse of FBF reserve to NG-monomethyl-L-arginine.
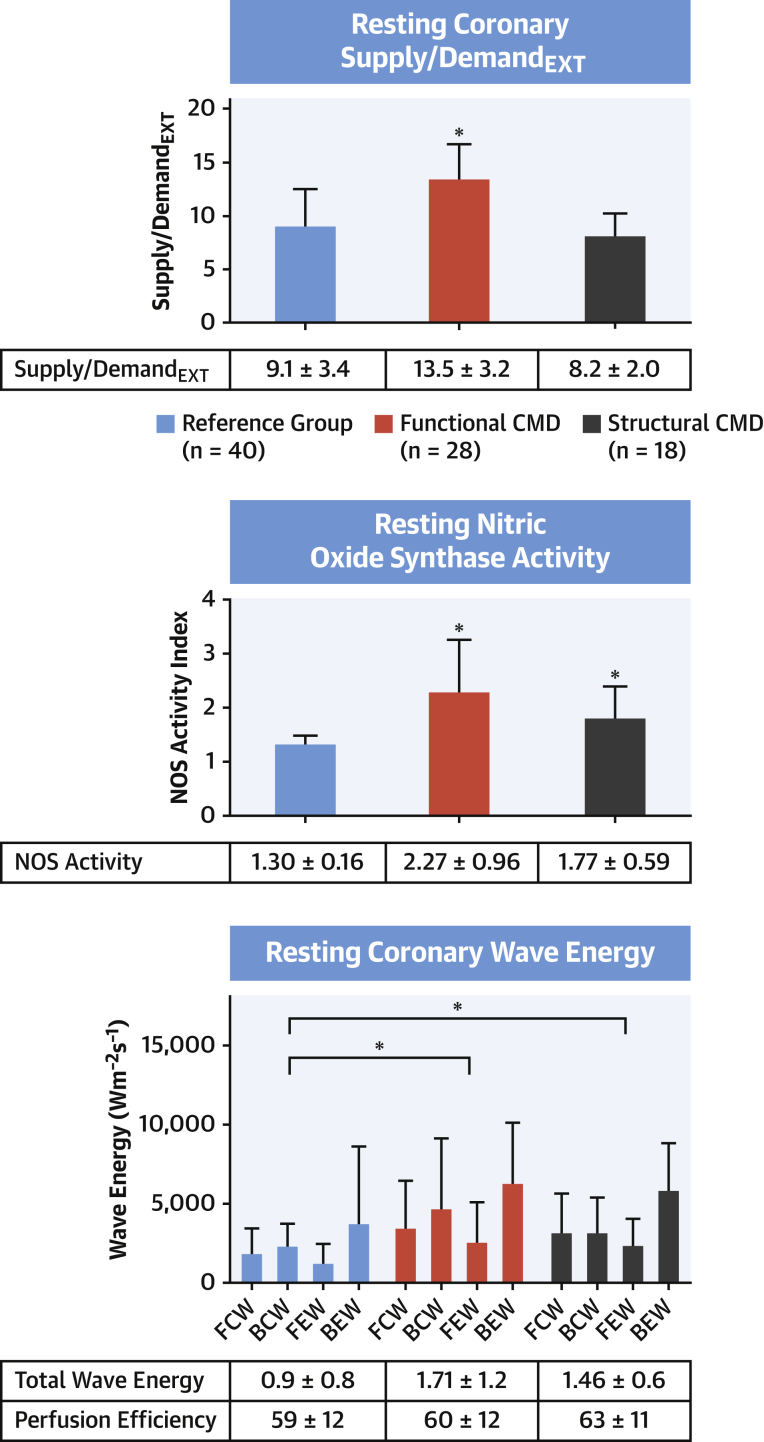
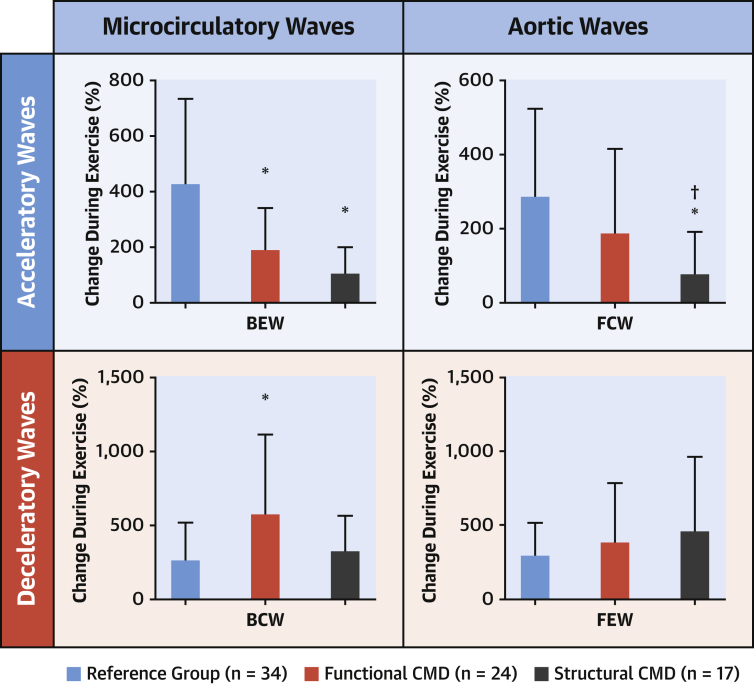
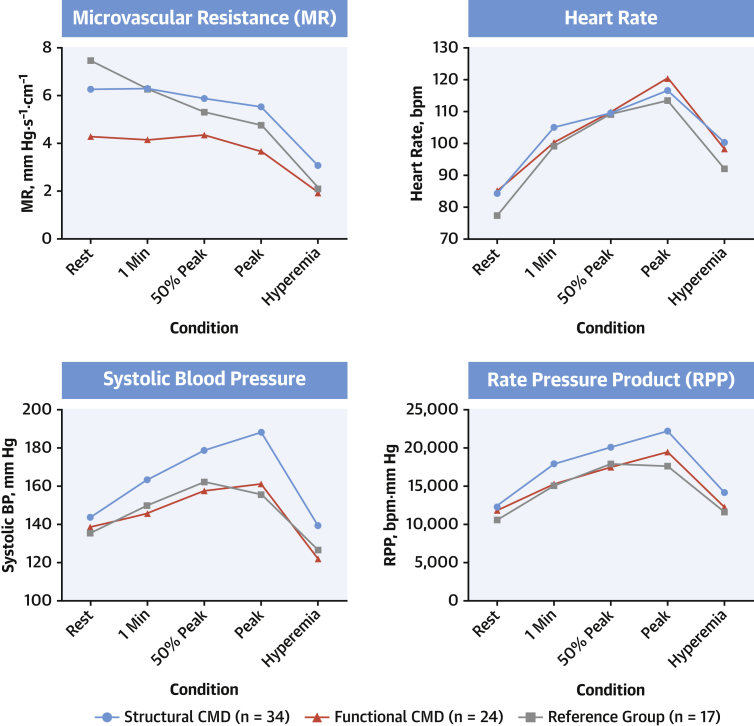
Results: Of the 86 patients, 46 had CMD (28 functional, 18 structural), and 40 patients formed the reference group. Resting coronary blood flow (CBF) (24.6 ± 2.0 cm/s vs. 16.6 ± 3.9 cm/s vs. 15.1 ± 4.7 cm/s; p < 0.001) and NOS activity (2.27 ± 0.96 vs. 1.77 ± 0.59 vs. 1.30 ± 0.16; p < 0.001) were higher in the functional group compared with the structural CMD and reference groups, respectively. The structural group had lower acetylcholine FBF augmentation than the functional or reference group (2.1 ± 1.8 vs. 4.1 ± 1.7 vs. 4.5 ± 2.0; p < 0.001). On exercise, oxygen demand was highest (rate-pressure product: 22,157 ± 5,497 beats/min/mm Hg vs. 19,519 ± 4,653 beats/min/mm Hg vs. 17,530 ± 4,678 beats/min/mm Hg; p = 0.004), but peak CBF was lowest in patients with structural CMD compared with the functional and reference groups.
Conclusions: Functional CMD is characterized by elevated resting flow that is linked to enhanced NOS activity. Patients with structural CMD have endothelial dysfunction, which leads to diminished peak CBF augmentation and increased demand during exercise. The value of pathophysiologically stratified therapy warrants investigation.
Keywords: coronary flow reserve; endothelial dysfunction; microvascular dysfunction; nitric oxide; stratified medicine.
Copyright © 2020 The Authors. Published by Elsevier Inc. All rights reserved.
Figures
Comment in
-
Invasive Functional Assessment in Patients With Angina and Coronary Microvascular Dysfunction: A Plea for More.J Am Coll Cardiol. 2020 May 26;75(20):2550-2552. doi: 10.1016/j.jacc.2020.03.052. J Am Coll Cardiol. 2020. PMID: 32439004 No abstract available.
References
-
- Pepine C.J., Anderson R.D., Sharaf B.L. Coronary microvascular reactivity to adenosine predicts adverse outcome in women evaluated for suspected ischemia: results from the National Heart, Lung and Blood Institute. WISE (Women’s Ischemia Syndrome Evaluation) study. J Am Coll Cardiol. 2010;55:2825–2832. - PMC - PubMed
-
- Seddon M., Melikian N., Dworakowski R. Effects of neuronal nitric oxide synthase on human coronary artery diameter and blood flow in vivo. Circulation. 2009;119:2656–2662. - PubMed
-
- Seddon M.D., Chowienczyk P.J., Brett S.E., Casadei B., Shah A.M. Neuronal nitric oxide synthase regulates basal microvascular tone in humans in vivo. Circulation. 2008;117:1991–1996. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
