

Modelling the cost-effectiveness of introducing subsidised malaria rapid diagnostic tests in the private retail sector in sub-Saharan Africa
- PMID: 32439690
- PMCID: PMC7247415
- DOI: 10.1136/bmjgh-2019-002138
Modelling the cost-effectiveness of introducing subsidised malaria rapid diagnostic tests in the private retail sector in sub-Saharan Africa
Abstract
Background: Over the last 10 years, there has been a huge shift in malaria diagnosis in public health facilities, due to widespread deployment of rapid diagnostic tests (RDTs), which are accurate, quick and easy to use and inexpensive. There are calls for RDTs to be made available at-scale in the private retail sector where many people with suspected malaria seek care. Retail sector RDT use in sub-Saharan Africa (SSA) is limited to small-scale studies, and robust evidence on value-for-money is not yet available. We modelled the cost-effectiveness of introducing subsidised RDTs and supporting interventions in the SSA retail sector, in a context of a subsidy programme for first-line antimalarials.
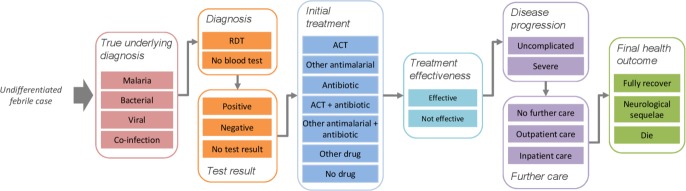
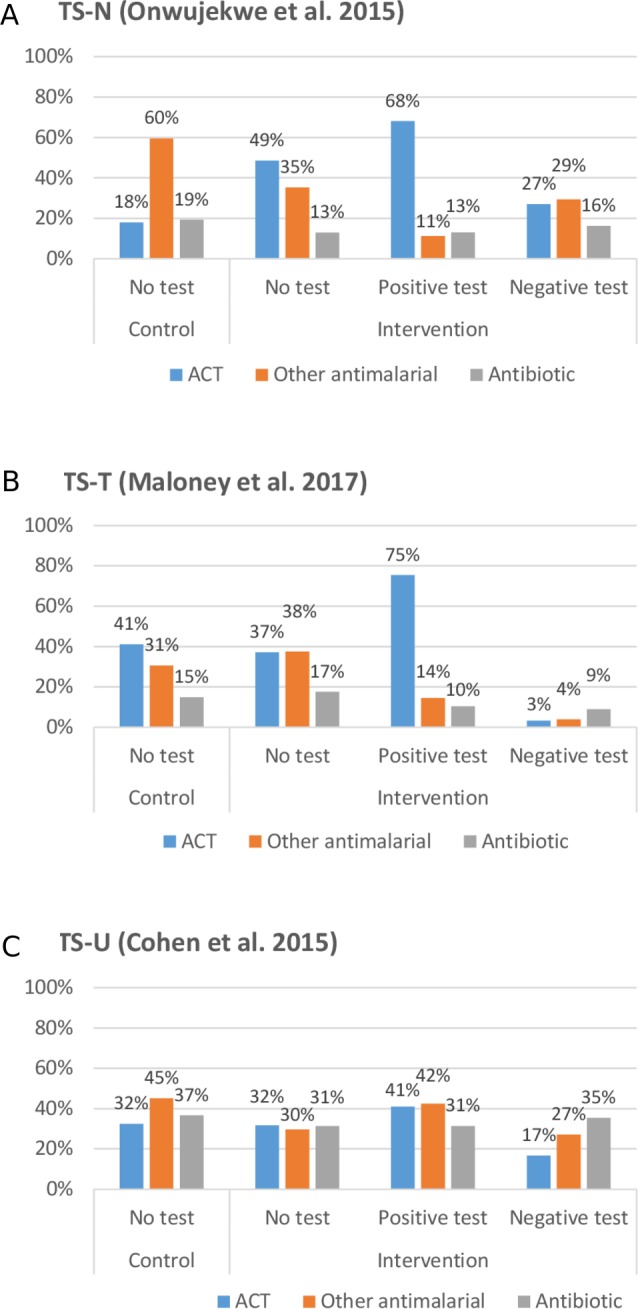
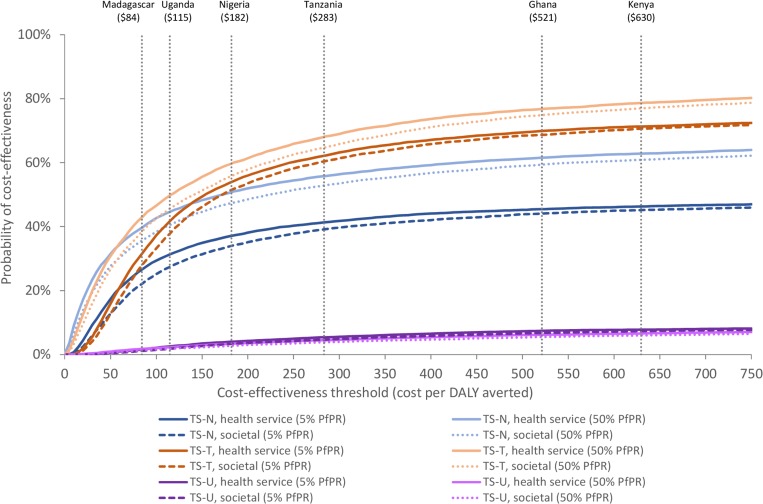
Methods: We developed a decision tree following febrile patients through presentation, diagnosis, treatment, disease progression and further care, to final health outcomes. We modelled results for three 'treatment scenarios', based on parameters from three small-scale studies in Nigeria (TS-N), Tanzania (TS-T) and Uganda (TS-U), under low and medium/high transmission (5% and 50% Plasmodium falciparum (parasite) positivity rates (PfPR), respectively).
Results: Cost-effectiveness varied considerably between treatment scenarios. Cost per disability-adjusted life year averted at 5% PfPR was US$482 (TS-N) and US$115 (TS-T) and at 50% PfPR US$44 (TS-N) and US$45 (TS-T), from a health service perspective. TS-U was dominated in both transmission settings.
Conclusion: The cost-effectiveness of subsidised RDTs is strongly influenced by treatment practices, for which further evidence is required from larger-scale operational settings. However, subsidised RDTs could promote increased use of first-line antimalarials in patients with malaria. RDTs may, therefore, be more cost-effective in higher transmission settings, where a greater proportion of patients have malaria and benefit from increased antimalarial use. This is contrary to previous public sector models, where RDTs were most cost-effective in lower transmission settings as they reduced unnecessary antimalarial use in patients without malaria.
Keywords: diagnostics and tools; health economics; malaria.
© Author(s) (or their employer(s)) 2020. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: None declared.
Figures
References
-
- World Health Organization Malaria case management operations manual 2009.
-
- World Health Organization World malaria report. Geneva: WHO, 2017.
-
- World Health Organization World malaria report. Geneva: WHO, 2018.
-
- AMFm Independent Evaluation Team Independent Evaluation of Phase 1 of the Affordable Medicines Facility - malaria (AMFm), Multi-Country Independent Evaluation Report: Final Report. Calverton, Maryland and London: ICF International and London School of Hygiene and Tropical Medicine, 2012.
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
Research Materials