

Reflux symptoms and oesophageal acidification in treated achalasia patients are often not reflux related
- PMID: 32439713
- PMCID: PMC7788183
- DOI: 10.1136/gutjnl-2020-320772
Reflux symptoms and oesophageal acidification in treated achalasia patients are often not reflux related
Abstract
Objective: After treatment, achalasia patients often develop reflux symptoms. Aim of this case-control study was to investigate mechanisms underlying reflux symptoms in treated achalasia patients by analysing oesophageal function, acidification patterns and symptom perception.
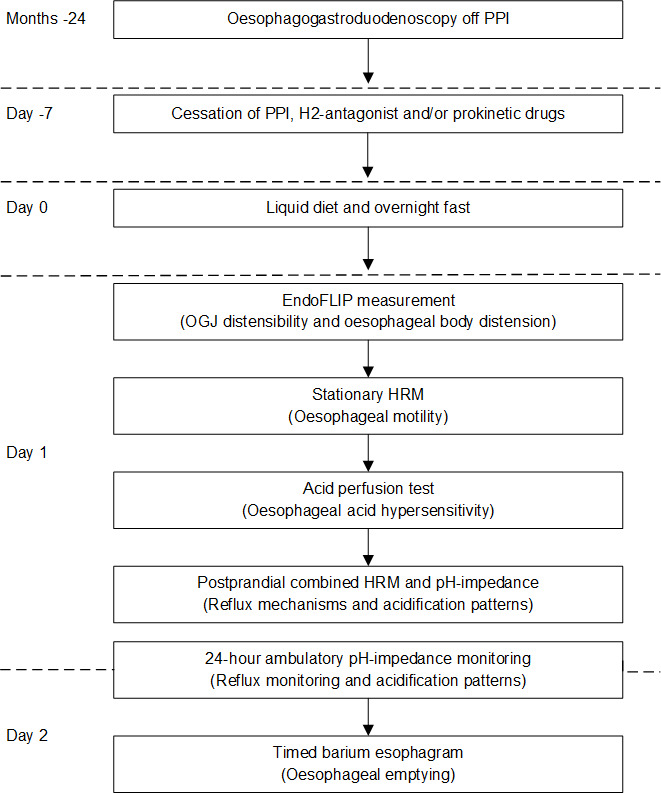
Design: Forty treated achalasia patients (mean age 52.9 years; 27 (68%) men) were included, 20 patients with reflux symptoms (RS+; Gastro-Oesophageal Reflux Disease Questionnaire (GORDQ) ≥8) and 20 without reflux symptoms (RS-: GORDQ <8). Patients underwent measurements of oesophagogastric junction distensibility, high-resolution manometry, timed barium oesophagogram, 24 hours pH-impedance monitoring off acid-suppression and oesophageal perception for acid perfusion and distension. Presence of oesophagitis was assessed endoscopically.
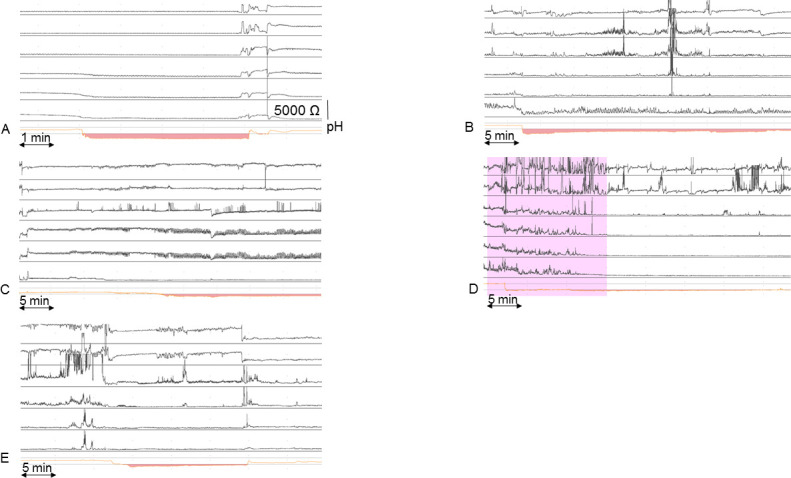
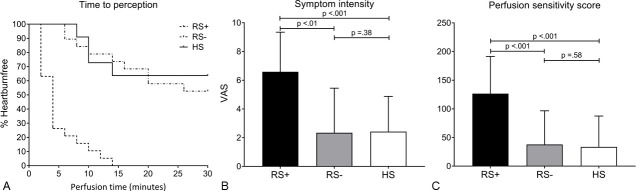
Results: Total acid exposure time during 24 hours pH-impedance was not significantly different between patients with (RS+) and without (RS-) reflux symptoms. In RS+ patients, acid fermentation was higher than in RS- patients (RS+: mean 6.6% (95% CI 2.96% to 10.2%) vs RS-: 1.8% (95% CI -0.45% to 4.1%, p=0.03) as well as acid reflux with delayed clearance (RS+: 6% (95% CI 0.94% to 11%) vs RS-: 3.4% (95% CI -0.34% to 7.18%), p=0.051). Reflux symptoms were not related to acid in both groups, reflected by a low Symptom Index. RS+ patients were highly hypersensitive to acid, with a much shorter time to heartburn perception (RS+: 4 (2-6) vs RS-:30 (14-30) min, p<0.001) and a much higher symptom intensity (RS+: 7 (4.8-9) vs RS-: 0.5 (0-4.5) Visual Analogue Scale, p<0.001) during acid perfusion. They also had a lower threshold for mechanical stimulation.
Conclusion: Reflux symptoms in treated achalasia are rarely caused by gastro-oesophageal reflux and most instances of oesophageal acidification are not reflux related. Instead, achalasia patients with post-treatment reflux symptoms demonstrate oesophageal hypersensitivity to chemical and mechanical stimuli, which may determine symptom generation.
Keywords: achalasia; gastroesophageal reflux disease; oesophageal motility disorder; oesophageal ph monitoring; visceral hypersensitivity.
© Author(s) (or their employer(s)) 2021. Re-use permitted under CC BY. Published by BMJ.
Conflict of interest statement
Competing interests: FAP: None. JMO: Received speaker and/or consulting fees from Laborie. AJS: None. AJB: Received research funding from Nutricia, Norgine and Bayer and received speaker and/or consulting fees from Laborie, EsoCap, Diversatek, Medtronic, Falk Pharma, Calypso Biotech, Thelial, Robarts, Reckett Benkiser, Regeneron, Celgene, Bayer, Norgine, AstraZeneca, Almirall, Arena and Allergan.
Figures
Similar articles
-
[The value of twenty-four hour intraoesophageal pH monitoring and manometry in the management of patients with upper gastrointestinal symptoms].Orv Hetil. 2009 Oct 25;150(43):1978-82. doi: 10.1556/OH.2009.28735. Orv Hetil. 2009. PMID: 19812019 Hungarian.
-
Effect of pneumatic dilation on gastroesophageal reflux in achalasia.Dig Dis Sci. 1997 May;42(5):998-1002. doi: 10.1023/a:1018884919125. Dig Dis Sci. 1997. PMID: 9149054
-
The relationship between gastro-oesophageal reflux symptoms and achalasia.Eur J Gastroenterol Hepatol. 2006 Apr;18(4):369-74. doi: 10.1097/00042737-200604000-00009. Eur J Gastroenterol Hepatol. 2006. PMID: 16538107
-
Post-per-oral endoscopic myotomy heartburn: It's not always reflux: Expert review.Dig Endosc. 2022 Jan;34(2):325-333. doi: 10.1111/den.14106. Epub 2021 Sep 1. Dig Endosc. 2022. PMID: 34390053 Review.
-
Utility of non-endoscopic investigations in the practical management of oesophageal disorders.Best Pract Res Clin Gastroenterol. 2009;23(3):369-86. doi: 10.1016/j.bpg.2009.03.005. Best Pract Res Clin Gastroenterol. 2009. PMID: 19505665 Review.
Cited by
-
Esophageal hyposensitivity in achalasia cardia: Do we finally have an answer?United European Gastroenterol J. 2020 Nov;8(9):1128-1129. doi: 10.1177/2050640620959156. Epub 2020 Sep 10. United European Gastroenterol J. 2020. PMID: 33151834 Free PMC article. No abstract available.
-
No advantage of fundoplication in paraesophageal hernia repair: a retrospective multicenter study.Dis Esophagus. 2025 May 3;38(3):doaf036. doi: 10.1093/dote/doaf036. Dis Esophagus. 2025. PMID: 40382786 Free PMC article.
-
Third-space endoscopy: the final frontier.Gastroenterol Rep (Oxf). 2023 Jan 10;11:goac077. doi: 10.1093/gastro/goac077. eCollection 2023. Gastroenterol Rep (Oxf). 2023. PMID: 36632624 Free PMC article. Review.
-
Prediction, prevention and management of gastroesophageal reflux after per-oral endoscopic myotomy: An update.World J Gastroenterol. 2024 Mar 7;30(9):1096-1107. doi: 10.3748/wjg.v30.i9.1096. World J Gastroenterol. 2024. PMID: 38577183 Free PMC article. Review.
-
Prevalence of Gastroesophageal Reflux Symptoms Post Sleeve Gastrectomy in Al-Qassim Region.Cureus. 2023 Aug 24;15(8):e44040. doi: 10.7759/cureus.44040. eCollection 2023 Aug. Cureus. 2023. PMID: 37746463 Free PMC article.
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical