

Long-term changes and effect of pterygium size on corneal topographic irregularity after recurrent pterygium surgery
- PMID: 32439899
- PMCID: PMC7242432
- DOI: 10.1038/s41598-020-65376-4
Long-term changes and effect of pterygium size on corneal topographic irregularity after recurrent pterygium surgery
Abstract
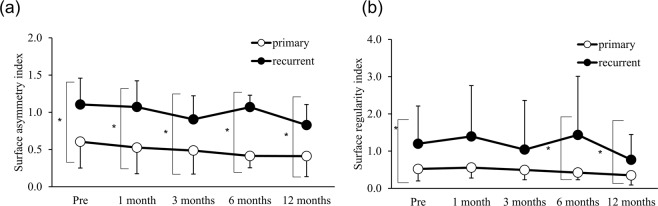
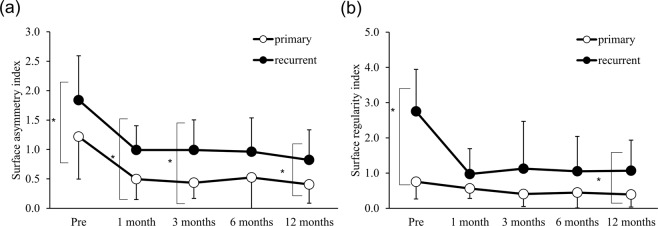
This retrospective observational study compared long-term topographic changes after recurrent- and primary-pterygium surgery depending on pterygium size. Patients who underwent recurrent-pterygium excision between 2002-2013 and age, sex, and pterygium size-matched controls who underwent primary-pterygium surgery were included (33 eyes of 33 patients in each group). Pterygium size was graded per advancing edge position: <1/3 of corneal diameter (grade 1), outside the pupil (grade 2), and within the pupillary area (grade 3). Surface asymmetry index (SAI), surface regularity index (SRI) in corneal topography, and uncorrected and best-spectacle-corrected visual acuity were compared before and 1, 3, 6, and 12 months postoperatively. Three, 17, and 13 eyes had grades 1, 2, and 3, respectively. In grade 2, the SAI and SRI were respectively significantly larger at all observation points (p = 0.01, 0.03, 0.02, 0.02, and 0.004) and before and 6 and 12 months postoperatively (p = 0.02, 0.04, and 0.03) in recurrent pterygium. In grade 3, the SAI was significantly larger before and 1, 3, and 12 months postoperatively (p = 0.04, 0.01, 0.01, and 0.02) and the SRI was significantly larger before and 12 months postoperatively (p < 0.001, 0.02) in recurrent pterygium. Corneal irregularity persisted 12 months after recurrent-pterygium surgery compared with that in same-size primary pterygium.
Conflict of interest statement
The authors declare no competing interests regarding this research.
Figures
References
Publication types
MeSH terms
Supplementary concepts
LinkOut - more resources
Full Text Sources
