

Restrictive intraoperative fluid management was associated with higher incidence of composite complications compared to less restrictive strategies in open thoracotomy: A retrospective cohort study
- PMID: 32439944
- PMCID: PMC7242459
- DOI: 10.1038/s41598-020-65532-w
Restrictive intraoperative fluid management was associated with higher incidence of composite complications compared to less restrictive strategies in open thoracotomy: A retrospective cohort study
Abstract
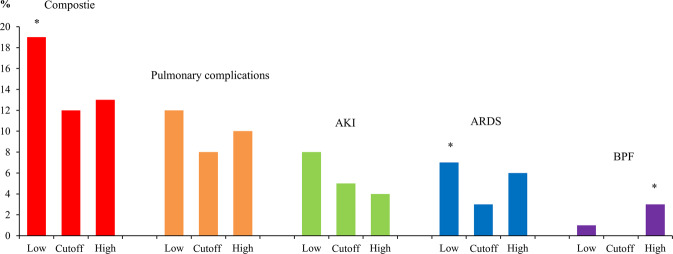
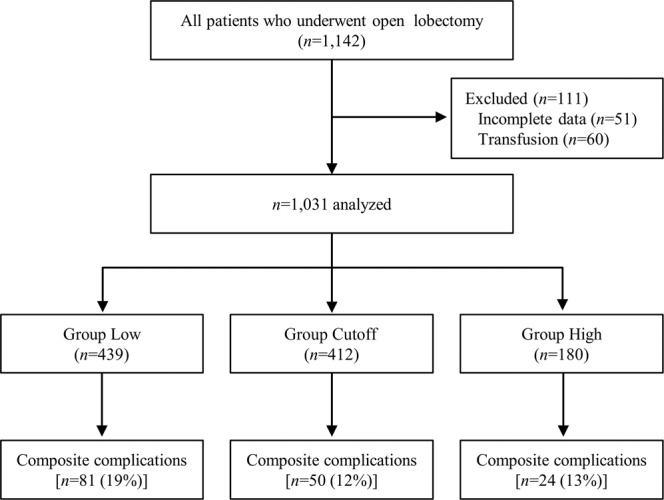
Restrictive fluid management has been recommended for thoracic surgery. However, specific guidelines are lacking, and there is always concern regarding impairment of renal perfusion with a restrictive policy. The objective of this study was to find the net intraoperative fluid infusion rate which shows the lowest incidence of composite complications (either pulmonary complications or acute kidney injury) in open thoracotomy. We hypothesized that a certain range of infusion rate would decrease the composite complications within postoperative 30 days. All patients (n = 1,031) who underwent open thoracotomy at a tertiary care university hospital were included in this retrospective study. The time frame of fluid monitoring was from the start of operation to postoperative 24 hours. The cutoff value of the intraoperative net fluid amount was 4-5 ml.kg-1.h-1 according to the minimum p-value method, thus, patients were divided into Low (≤3 ml.kg-1.h-1), Cutoff (4-5 ml.kg-1.h-1) and High (≥6 ml.kg-1.h-1) groups. The Cutoff group showed the lowest composite complication rate (19%, 12%, and 13% in the Low, Cutoff, and High groups, respectively, P = 0.0283; Low vs. Cutoff, P = 0.0324, Bonferroni correction). Acute respiratory distress syndrome occurred least frequently in the Cutoff group (7%, 3%, and 6% for the Low, Cutoff, and High groups, respectively, P = 0.0467; Low vs. Cutoff, P = 0.0432, Bonferroni correction). In multivariable analysis, intraoperative net fluid infusion rate was associated with composite complications, and the Cutoff group decreased risk (odds ratio 0.54, 95% confidence interval: 0.35-0.81, P = 0.0035). In conclusion, maintaining intraoperative net fluid infusion at 4-5 ml.kg-1.h-1 was associated with better results in open thoracotomy, in terms of composite complications, compared to more restrictive fluid management.
Conflict of interest statement
The authors declare no competing interests.
Figures
References
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
