

Best Local Flaps for Lower Extremity Reconstruction
- PMID: 32440438
- PMCID: PMC7209892
- DOI: 10.1097/GOX.0000000000002774
Best Local Flaps for Lower Extremity Reconstruction
Abstract
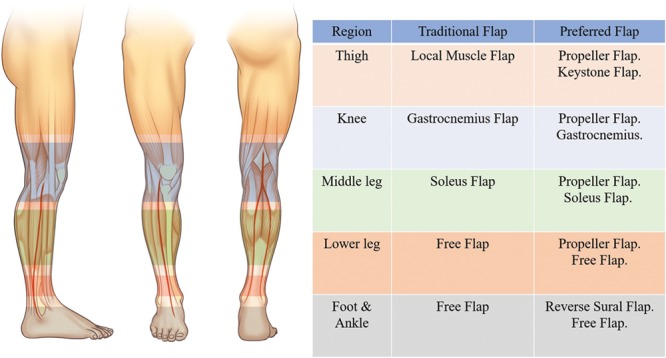
The ideal reconstruction of lower limb defects should replace like with like and minimize morbidity to the donor site, achieving the best possible esthetic and functional outcome. The goal is to obtain stable healing and to resume daily life in an efficient manner. Although the classical local flaps such as gastrocnemius, soleus muscle flap, and the reverse sural flap have allowed to achieve those goals, perforator flaps are now added on to the armamentarium in lower extremity reconstruction using local flaps. A perforator-based local flap, such as a propeller or keystone flap, has made reconstruction efficient while further reducing donor-site morbidity. This article aims to provide a useful review of the best available local flaps for lower limb defects.
Copyright © 2020 The Authors. Published by Wolters Kluwer Health, Inc. on behalf of The American Society of Plastic Surgeons.
Conflict of interest statement
Disclosure: The authors have no financial interest to declare in relation to the content of this article.
Figures





References
-
- Soltanian H, Garcia RM, Hollenbeck ST. Current concepts in lower extremity reconstruction. Plast Reconstr Surg. 2015;136:815e–829e. - PubMed
-
- Hallock GG. A paradigm shift in flap selection protocols for zones of the lower extremity using perforator flaps. J Reconstr Microsurg. 2013;29:233–240. - PubMed
-
- Nelson JA, Fischer JP, Brazio PS, et al. A review of propeller flaps for distal lower extremity soft tissue reconstruction: is flap loss too high? Microsurgery. 2013;33:578–586. - PubMed
-
- Hollenbeck ST, Toranto JD, Taylor BJ, et al. Perineal and lower extremity reconstruction. Plast Reconstr Surg. 2011;128:551e–563e. - PubMed
-
- Hallock GG. Local fasciocutaneous flaps for cutaneous coverage of lower extremity wounds. J Trauma. 1989;29:1240–1244. - PubMed
Publication types
LinkOut - more resources
Full Text Sources