

An overview of management of intracranial hypertension in the intensive care unit
- PMID: 32440802
- PMCID: PMC7241587
- DOI: 10.1007/s00540-020-02795-7
An overview of management of intracranial hypertension in the intensive care unit
Abstract
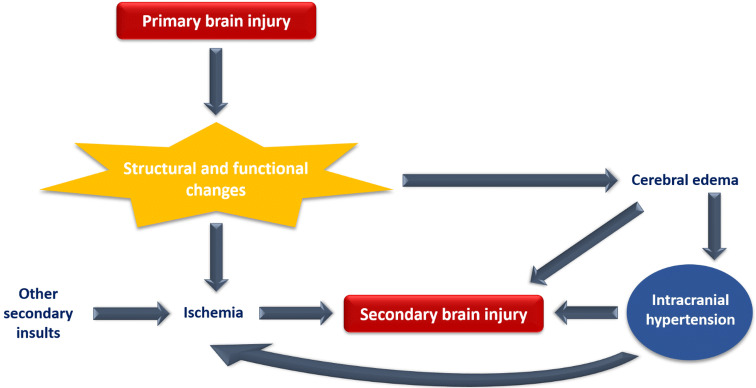
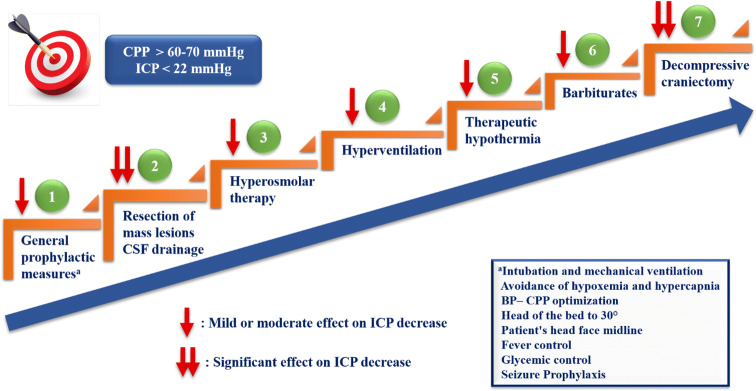
Intracranial hypertension (IH) is a clinical condition commonly encountered in the intensive care unit, which requires immediate treatment. The maintenance of normal intracranial pressure (ICP) and cerebral perfusion pressure in order to prevent secondary brain injury (SBI) is the central focus of management. SBI can be detected through clinical examination and invasive and non-invasive ICP monitoring. Progress in monitoring and understanding the pathophysiological mechanisms of IH allows the implementation of targeted interventions in order to improve the outcome of these patients. Initially, general prophylactic measures such as patient's head elevation, fever control, adequate analgesia and sedation depth should be applied immediately to all patients with suspected IH. Based on specific indications and conditions, surgical resection of mass lesions and cerebrospinal fluid drainage should be considered as an initial treatment for lowering ICP. Hyperosmolar therapy (mannitol or hypertonic saline) represents the cornerstone of medical treatment of acute IH while hyperventilation should be limited to emergency management of life-threatening raised ICP. Therapeutic hypothermia could have a possible benefit on outcome. To control elevated ICP refractory to maximum standard medical and surgical treatment, at first, high-dose barbiturate administration and then decompressive craniectomy as a last step are recommended with unclear and probable benefit on outcomes, respectively. The therapeutic strategy should be based on a staircase approach and be individualized for each patient. Since most therapeutic interventions have an uncertain effect on neurological outcome and mortality, future research should focus on both studying the long-term benefits of current strategies and developing new ones.
Keywords: Cerebral perfusion pressure; Intracranial hypertension; Intracranial pressure; Neurocritical care; Osmotic agents; Traumatic brain injury.
Conflict of interest statement
The authors have no conflict of interest.
Figures
References
-
- Le Roux P, Menon DK, Citerio G, Vespa P, Bader MK, Brophy GM, Diringer MN, Stocchetti N, Videtta W, Armonda R, Badjatia N, Böesel J, Chesnut R, Chou S, Claassen J, Czosnyka M, De Georgia M, Figaji A, Fugate J, Helbok R, Horowitz D, Hutchinson P, Kumar M, McNett M, Miller C, Naidech A, Oddo M, Olson D, O'Phelan K, Provencio JJ, Puppo C, Riker R, Robertson C, Schmidt M, Taccone F. Consensus summary statement of the International Multidisciplinary Consensus Conference on Multimodality Monitoring in Neurocritical Care: a statement for healthcare professionals from the Neurocritical Care Society and the European Society of Intensive Care Medicine. Neurocrit Care. 2014; 21(2):1–26. - PMC - PubMed
-
- Güiza F, Depreitere B, Piper I, Citerio G, Chambers I, Jones PA, Lo TY, Enblad P, Nillson P, Feyen B, Jorens P, Maas A, Schuhmann MU, Donald R, Moss L, Van den Berghe G, Meyfroidt G. Visualizing the pressure and time burden of intracranial hypertension in adult and paediatric traumatic brain injury. Intensive Care Med. 2015;41(6):1067–1076. - PubMed
-
- Carney N, Totten AM, OʼReilly C, Ullman JS, Hawryluk GW, Bell MJ, Bratton SL, Chesnut R, Harris OA, Kissoon N, Rubiano AM, Shutter L, Tasker RC, Vavilala MS, Wilberger J, Wright DW, Ghajar J. Guidelines for the Management of Severe Traumatic Brain Injury, Fourth Edition. Neurosurgery. 2017; 80(1):6–15. - PubMed
-
- Agrawal D, Raghavendran K, Schaubel DE, Mishra MC, Rajajee V. A propensity score analysis of the impact of invasive intracranial pressure monitoring on outcomes after severe traumatic brain injury. J Neurotrauma. 2016;33(9):853–858. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
