

Ventilation Techniques and Risk for Transmission of Coronavirus Disease, Including COVID-19: A Living Systematic Review of Multiple Streams of Evidence
- PMID: 32442035
- PMCID: PMC7281716
- DOI: 10.7326/M20-2306
Ventilation Techniques and Risk for Transmission of Coronavirus Disease, Including COVID-19: A Living Systematic Review of Multiple Streams of Evidence
Update in
-
Update Alert 3: Ventilation Techniques and Risk for Transmission of Coronavirus Disease, Including COVID-19.Ann Intern Med. 2022 Jan;175(1):W6-W7. doi: 10.7326/L21-0424. Epub 2021 Dec 14. Ann Intern Med. 2022. PMID: 34904866 Free PMC article. No abstract available.
Abstract
Background: Mechanical ventilation is used to treat respiratory failure in coronavirus disease 2019 (COVID-19).
Purpose: To review multiple streams of evidence regarding the benefits and harms of ventilation techniques for coronavirus infections, including that causing COVID-19.
Data sources: 21 standard, World Health Organization-specific and COVID-19-specific databases, without language restrictions, until 1 May 2020.
Study selection: Studies of any design and language comparing different oxygenation approaches in patients with coronavirus infections, including severe acute respiratory syndrome (SARS) or Middle East respiratory syndrome (MERS), or with hypoxemic respiratory failure. Animal, mechanistic, laboratory, and preclinical evidence was gathered regarding aerosol dispersion of coronavirus. Studies evaluating risk for virus transmission to health care workers from aerosol-generating procedures (AGPs) were included.
Data extraction: Independent and duplicate screening, data abstraction, and risk-of-bias assessment (GRADE for certainty of evidence and AMSTAR 2 for included systematic reviews).
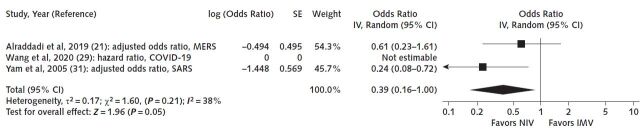
Data synthesis: 123 studies were eligible (45 on COVID-19, 70 on SARS, 8 on MERS), but only 5 studies (1 on COVID-19, 3 on SARS, 1 on MERS) adjusted for important confounders. A study in hospitalized patients with COVID-19 reported slightly higher mortality with noninvasive ventilation (NIV) than with invasive mechanical ventilation (IMV), but 2 opposing studies, 1 in patients with MERS and 1 in patients with SARS, suggest a reduction in mortality with NIV (very-low-certainty evidence). Two studies in patients with SARS report a reduction in mortality with NIV compared with no mechanical ventilation (low-certainty evidence). Two systematic reviews suggest a large reduction in mortality with NIV compared with conventional oxygen therapy. Other included studies suggest increased odds of transmission from AGPs.
Limitation: Direct studies in COVID-19 are limited and poorly reported.
Conclusion: Indirect and low-certainty evidence suggests that use of NIV, similar to IMV, probably reduces mortality but may increase the risk for transmission of COVID-19 to health care workers.
Primary funding source: World Health Organization. (PROSPERO: CRD42020178187).
Figures

Comment in
-
Update Alert: Ventilation Techniques and Risk for Transmission of Coronavirus Disease, Including COVID-19.Ann Intern Med. 2020 Sep 15;173(6):W122. doi: 10.7326/L20-0944. Epub 2020 Jul 31. Ann Intern Med. 2020. PMID: 32735446 Free PMC article. No abstract available.
-
Update Alert 2: Ventilation Techniques and Risk for Transmission of Coronavirus Disease, Including COVID-19.Ann Intern Med. 2020 Dec 1;173(11):W152-W153. doi: 10.7326/L20-1211. Epub 2020 Oct 13. Ann Intern Med. 2020. PMID: 33045175 Free PMC article. No abstract available.
-
Ventilation Techniques and Risk for Transmission of Coronavirus Disease, Including COVID-19.Ann Intern Med. 2020 Nov 17;173(10):860. doi: 10.7326/L20-1178. Ann Intern Med. 2020. PMID: 33197336 No abstract available.
References
-
- Coronavirus cases. Worldometer. Accessed at www.worldometers.info/coronavirus/ on 18 May 2020.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Miscellaneous