

Role of CD4/CD8 ratio on the incidence of tuberculosis in HIV-infected patients on antiretroviral therapy followed up for more than a decade
- PMID: 32442166
- PMCID: PMC7244128
- DOI: 10.1371/journal.pone.0233049
Role of CD4/CD8 ratio on the incidence of tuberculosis in HIV-infected patients on antiretroviral therapy followed up for more than a decade
Abstract
Background: The role of CD4/CD8 ratio on the incidence of tuberculosis (TB) in patients on antiretroviral therapy (ART) is unknown. Thus, we sought to determine whether the CD4/CD8 ratio was associated with development of TB in a cohort of HIV infected individuals on ART followed up for more than a decade in the setting of sub-Saharan Africa (SSA).
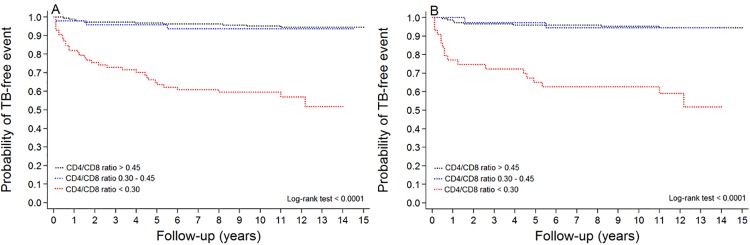
Methods: The cohort comprised adult patients who started ART between 2001 and 2007 and followed for up to 15 years. Clinical data were collected in retrospective manner. Patients with an AIDS defining illness or a CD4 count <200 cell/μL were started with a combination of ART. The participants have clinic visits every 6 months and/or as needed. Poisson regression models were used to identify factors associated with development of incident TB. Kaplan-Meier curves were used to estimate the probability of incident TB while on ART.
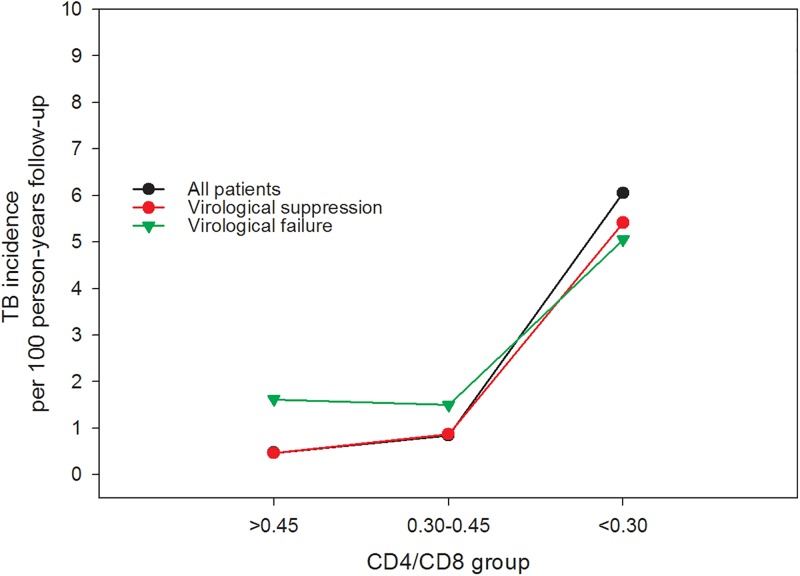
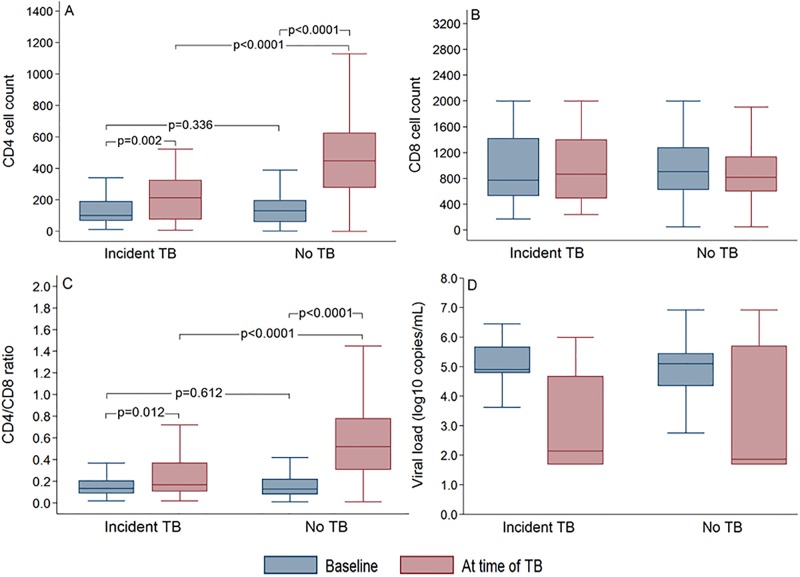
Results: A total of 347 patients with a median duration of follow-up on ART of 11.5 (IQR: 10.0-12.5) years were included. Incident TB developed in 47 patients during the 3259 person-years of follow-up, the majority (76.6%) occurred within five year of ART initiation. On univariate analysis, poor ART adherence (RR:2.57, 95% CI: 1.28-5.17), time-updated CD4 cell count of lower than 200 (RR: 4.86, 95%CI 2.33-10.15), or CD4 cell count between 200 and 500 (RR: 4.68, 95% CI: 2.17-10.09), time-updated CD8 cell count lower than 500 (RR: 2.83 95% CI 1.31-6.10), or CD8 cell count over 1000 (RR: 2.23, 95% CI: 1.12-4.45), time-updated CD4/CD8 ratio of less than 0.30 (RR: 6.00, 95% CI: 2.96-12.14), lack of normalization of CD4 T-cell count (RR: 6.13, 95% CI: 2.20-17.07), and virological failure (RR: 2.35 (95% CI: 1.17-4.71) were all associated with increased risk of incident TB. In multivariate analysis, however, time-updated CD4/CD8 ratio of less than 0.30 (adjusted RR: 4.08, 95% CI: 1.31-12.68) was the only factor associated with increased risk of developing incident TB (p = 0.015). Similar results were obtained in a sensitivity analysis by including only those virally suppressed patients (n = 233, 69% of all patients). In this group, CD4/CD8 ratio of less than 0.30 was associated with development of incident TB (adjusted RR: 4.02, 95% CI: 1.14-14.19, p = 0.031). Overall, the incidence rate of TB in patients with an updated CD4/CD8 ratio of less than 0.30 was more than 5-fold higher when compared with those with a ratio more than 0.45.
Conclusion: Low CD4/CD8 ratio is independently associated with an increased risk of incident TB despite viral suppression. CD4/CD8 ratio may serve as a biomarker for identifying patients at risk of TB in patients on ART in the setting of SSA.
Conflict of interest statement
The authors have declared that no competing interests exist.
Figures
Similar articles
-
Immune recovery in HIV-1 infected patients with sustained viral suppression under long-term antiretroviral therapy in Ethiopia.PLoS One. 2020 Oct 22;15(10):e0240880. doi: 10.1371/journal.pone.0240880. eCollection 2020. PLoS One. 2020. PMID: 33091053 Free PMC article.
-
Incident tuberculosis during antiretroviral therapy contributes to suboptimal immune reconstitution in a large urban HIV clinic in sub-Saharan Africa.PLoS One. 2010 May 7;5(5):e10527. doi: 10.1371/journal.pone.0010527. PLoS One. 2010. PMID: 20479873 Free PMC article.
-
CD4/CD8 ratio normalization rates and low ratio as prognostic marker for non-AIDS defining events among long-term virologically suppressed people living with HIV.AIDS Res Ther. 2018 Sep 27;15(1):13. doi: 10.1186/s12981-018-0200-4. AIDS Res Ther. 2018. PMID: 30261902 Free PMC article.
-
Tuberculosis and its association with CD4+ T cell count among adult HIV positive patients in Ethiopian settings: a systematic review and meta-analysis.BMC Infect Dis. 2020 May 7;20(1):325. doi: 10.1186/s12879-020-05040-4. BMC Infect Dis. 2020. PMID: 32380957 Free PMC article.
-
Tuberculosis associated mortality in a prospective cohort in Sub Saharan Africa: Association with HIV and antiretroviral therapy.Int J Infect Dis. 2017 Mar;56:39-44. doi: 10.1016/j.ijid.2017.01.023. Epub 2017 Feb 1. Int J Infect Dis. 2017. PMID: 28161460 Review.
Cited by
-
Immune recovery in HIV-1 infected patients with sustained viral suppression under long-term antiretroviral therapy in Ethiopia.PLoS One. 2020 Oct 22;15(10):e0240880. doi: 10.1371/journal.pone.0240880. eCollection 2020. PLoS One. 2020. PMID: 33091053 Free PMC article.
-
Autonomic Neuropathy Is Associated with An Increase in Type-1 Cytokines in People Living With HIV.bioRxiv [Preprint]. 2025 Apr 10:2024.10.15.618447. doi: 10.1101/2024.10.15.618447. bioRxiv. 2025. Update in: Clin Auton Res. 2025 Aug;35(4):567-580. doi: 10.1007/s10286-025-01129-5. PMID: 39464041 Free PMC article. Updated. Preprint.
-
Association of age at antiretroviral therapy initiation with CD4 + : CD8 + ratio recovery among virally suppressed people with HIV.AIDS. 2024 Apr 1;38(5):703-711. doi: 10.1097/QAD.0000000000003801. Epub 2024 Feb 26. AIDS. 2024. PMID: 38016172 Free PMC article.
-
No smoke without fire: the impact of cigarette smoking on the immune control of tuberculosis.Eur Respir Rev. 2022 Jun 7;31(164):210252. doi: 10.1183/16000617.0252-2021. Print 2022 Jun 30. Eur Respir Rev. 2022. PMID: 35675921 Free PMC article. Review.
-
Autonomic neuropathy is associated with an increase in type-1 cytokines in people living with HIV.Clin Auton Res. 2025 Aug;35(4):567-580. doi: 10.1007/s10286-025-01129-5. Epub 2025 May 10. Clin Auton Res. 2025. PMID: 40347412
References
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Medical
Research Materials
