

Muscle Mass Assessed by the D3-Creatine Dilution Method and Incident Self-reported Disability and Mortality in a Prospective Observational Study of Community-Dwelling Older Men
- PMID: 32442245
- PMCID: PMC7756711
- DOI: 10.1093/gerona/glaa111
Muscle Mass Assessed by the D3-Creatine Dilution Method and Incident Self-reported Disability and Mortality in a Prospective Observational Study of Community-Dwelling Older Men
Abstract
Background: Whether low muscle mass is a risk factor for disability and mortality is unclear. Associations between approximations of muscle mass (including lean mass from dual-energy x-ray absorptiometry [DXA]), and these outcomes are inconsistent.
Methods: Muscle mass measured by deuterated creatine (D3Cr) dilution and appendicular lean mass (ALM, by DXA) were assessed at the Year 14 Visit (2014-2016) of the prospective Osteoporotic Fractures in Men study (N = 1,425, age 77-101 years). Disability in activities of daily living (ADLs), instrumental ADLs, and mobility tasks was self-reported at the Year 14 visit and 2.2 years later; deaths were centrally adjudicated over 3.3 years. Relative risks and 95% confidence intervals (CI) were estimated per standard deviation decrement with negative binomial, logistic regression, or proportional hazards models.
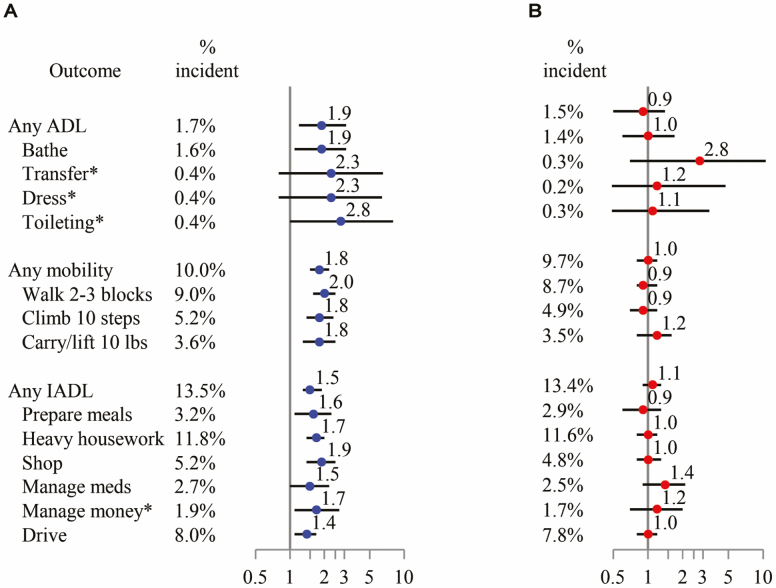
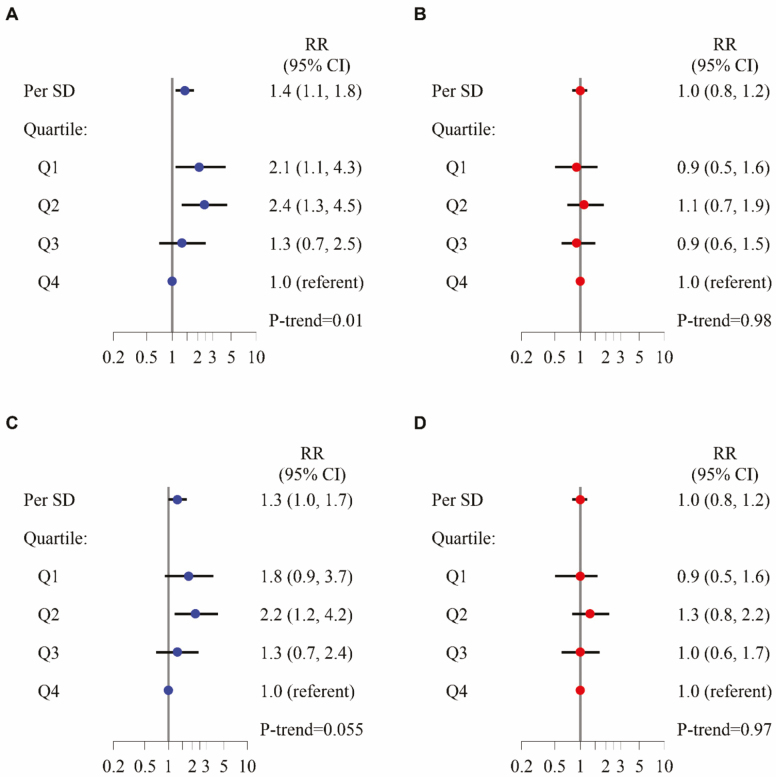
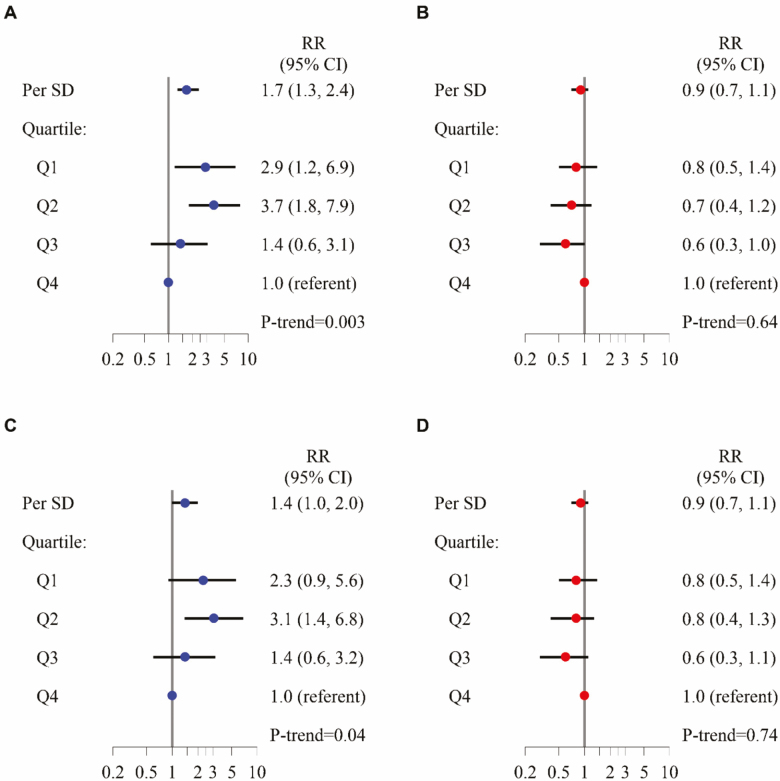
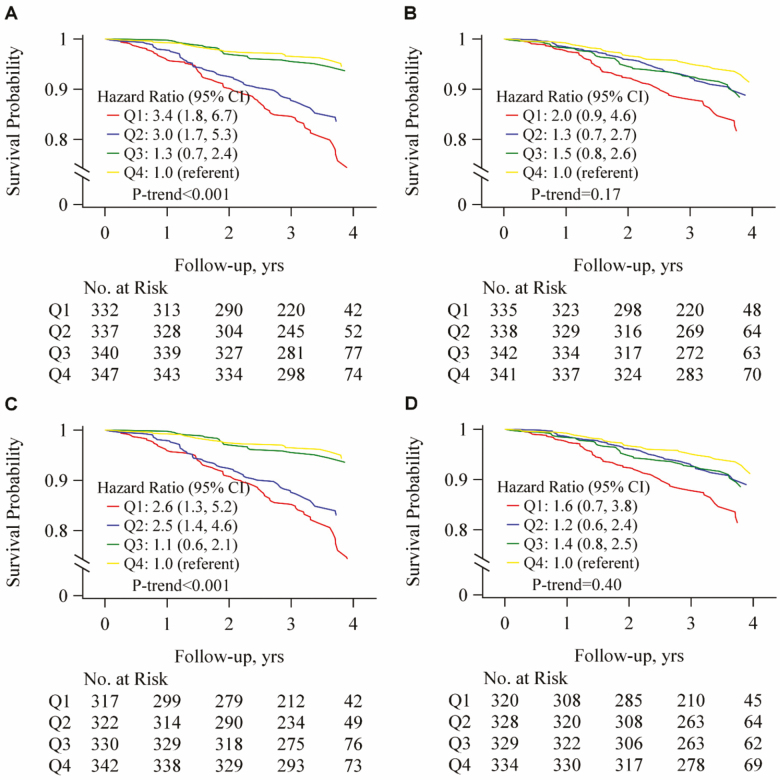
Results: In age- and clinical center-adjusted models, the relative risks per decrement in D3Cr muscle mass/wgt was 1.9 (95% CI: 1.2, 3.1) for incident self-reported ADL disability; 1.5 (95% CI: 1.3, 1.9) for instrumental ADL disability; and 1.8 (95% CI: 1.5, 2.2) for mobility disability. In age-, clinical center-, and weight-adjusted models, the relative risks per decrement in D3Cr muscle mass was 1.8 (95% CI: 1.5, 2.2) for all-cause mortality. In contrast, lower DXA ALM was not associated with any outcome. Associations of D3Cr muscle mass with these outcomes were slightly attenuated after adjustment for confounding factors and the potentially mediating effects of strength and physical performance.
Conclusions: Low muscle mass as measured by D3Cr dilution is a novel risk factor for clinically meaningful outcomes in older men.
Keywords: Death; Disability; Muscle mass.
© The Author(s) 2020. Published by Oxford University Press on behalf of The Gerontological Society of America. All rights reserved. For permissions, please e-mail: journals.permissions@oup.com.
Figures
References
-
- Wu Y, Wang W, Liu T, Zhang D. Association of grip strength with risk of all-cause mortality, cardiovascular diseases, and cancer in community-dwelling populations: a meta-analysis of prospective cohort studies. J Am Med Dir Assoc. 2017;18(6):551.e17–e35. doi: 10.1016/j.jamda.2017.03.011 - DOI - PubMed
