

Collateral damage: the impact on outcomes from cancer surgery of the COVID-19 pandemic
- PMID: 32442581
- PMCID: PMC7237184
- DOI: 10.1016/j.annonc.2020.05.009
Collateral damage: the impact on outcomes from cancer surgery of the COVID-19 pandemic
Abstract
Background: Cancer diagnostics and surgery have been disrupted by the response of health care services to the coronavirus disease 2019 (COVID-19) pandemic. Progression of cancers during delay will impact on patients' long-term survival.
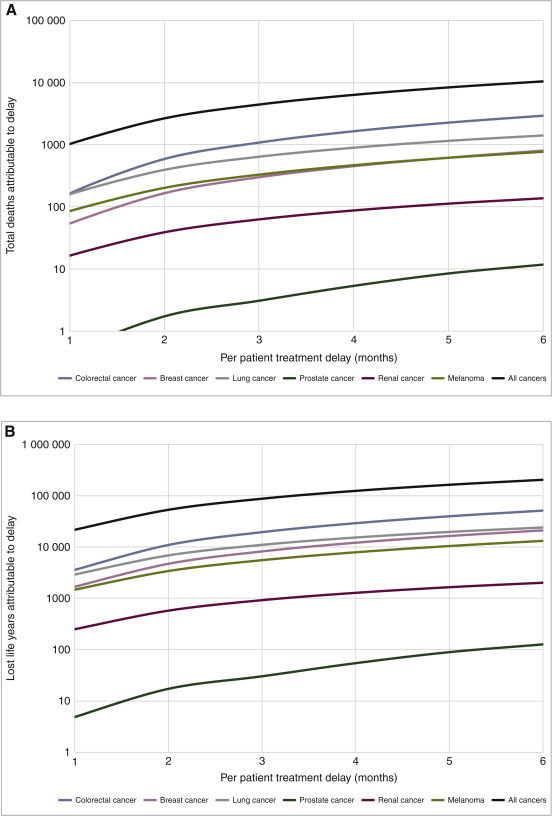
Patients and methods: We generated per-day hazard ratios of cancer progression from observational studies and applied these to age-specific, stage-specific cancer survival for England 2013-2017. We modelled per-patient delay of 3 and 6 months and periods of disruption of 1 and 2 years. Using health care resource costing, we contextualise attributable lives saved and life-years gained (LYGs) from cancer surgery to equivalent volumes of COVID-19 hospitalisations.
Results: Per year, 94 912 resections for major cancers result in 80 406 long-term survivors and 1 717 051 LYGs. Per-patient delay of 3/6 months would cause attributable death of 4755/10 760 of these individuals with loss of 92 214/208 275 life-years, respectively. For cancer surgery, average LYGs per patient are 18.1 under standard conditions and 17.1/15.9 with a delay of 3/6 months (an average loss of 0.97/2.19 LYGs per patient), respectively. Taking into account health care resource units (HCRUs), surgery results on average per patient in 2.25 resource-adjusted life-years gained (RALYGs) under standard conditions and 2.12/1.97 RALYGs following delay of 3/6 months. For 94 912 hospital COVID-19 admissions, there are 482 022 LYGs requiring 1 052 949 HCRUs. Hospitalisation of community-acquired COVID-19 patients yields on average per patient 5.08 LYG and 0.46 RALYGs.
Conclusions: Modest delays in surgery for cancer incur significant impact on survival. Delay of 3/6 months in surgery for incident cancers would mitigate 19%/43% of LYGs, respectively, by hospitalisation of an equivalent volume of admissions for community-acquired COVID-19. This rises to 26%/59%, respectively, when considering RALYGs. To avoid a downstream public health crisis of avoidable cancer deaths, cancer diagnostic and surgical pathways must be maintained at normal throughput, with rapid attention to any backlog already accrued.
Keywords: COVID-19; delay; diagnostics; oncology; survival.
Copyright © 2020 The Author(s). Published by Elsevier Ltd.. All rights reserved.
Conflict of interest statement
Disclosure The authors have declared no conflicts of interest.
Figures
References
-
- Cancer referrals fell from 40,000 to 10,000 per week in April. In NHS Providers 14/05/20. 2020.
-
- Updated Intercollegiate General Surgery Guidance on COVID-19. Royal College of Surgeons England; 2020.
-
- Endoscopy activity and COVID-19: British Society of Gastroenterology and Joint Advisory Group guidance – update 03.04.20. 2020.
-
- National Cancer Registration and Analysis Service (NCRAS) Public Health England; 2018.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
