

Pulmonary and systemic involvement in COVID-19 patients assessed with ultrasound-guided minimally invasive autopsy
- PMID: 32443177
- PMCID: PMC7280721
- DOI: 10.1111/his.14160
Pulmonary and systemic involvement in COVID-19 patients assessed with ultrasound-guided minimally invasive autopsy
Abstract
Aims: Brazil ranks high in the number of coronavirus disease 19 (COVID-19) cases and the COVID-19 mortality rate. In this context, autopsies are important to confirm the disease, determine associated conditions, and study the pathophysiology of this novel disease. The aim of this study was to assess the systemic involvement of COVID-19. In order to follow biosafety recommendations, we used ultrasound-guided minimally invasive autopsy (MIA-US), and we present the results of 10 initial autopsies.
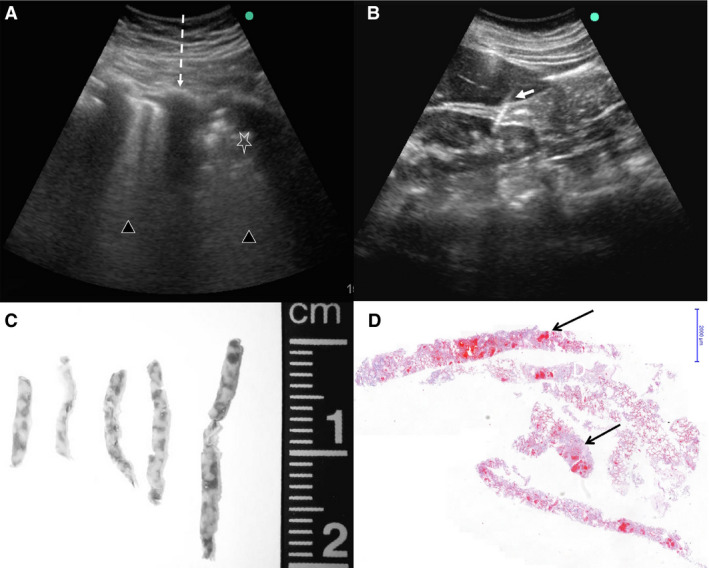
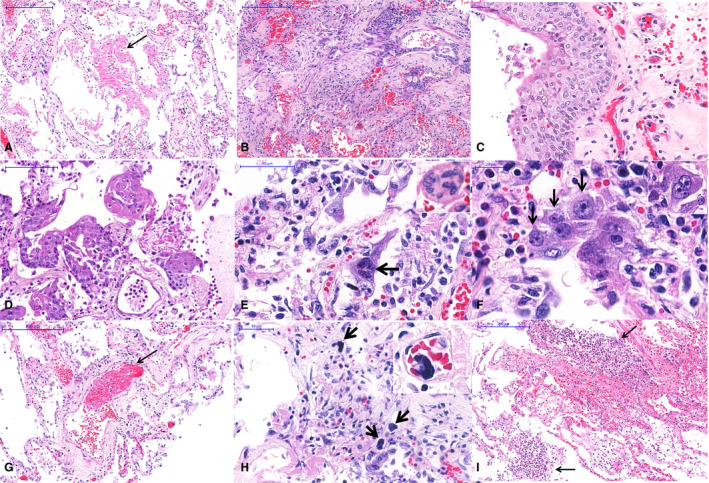
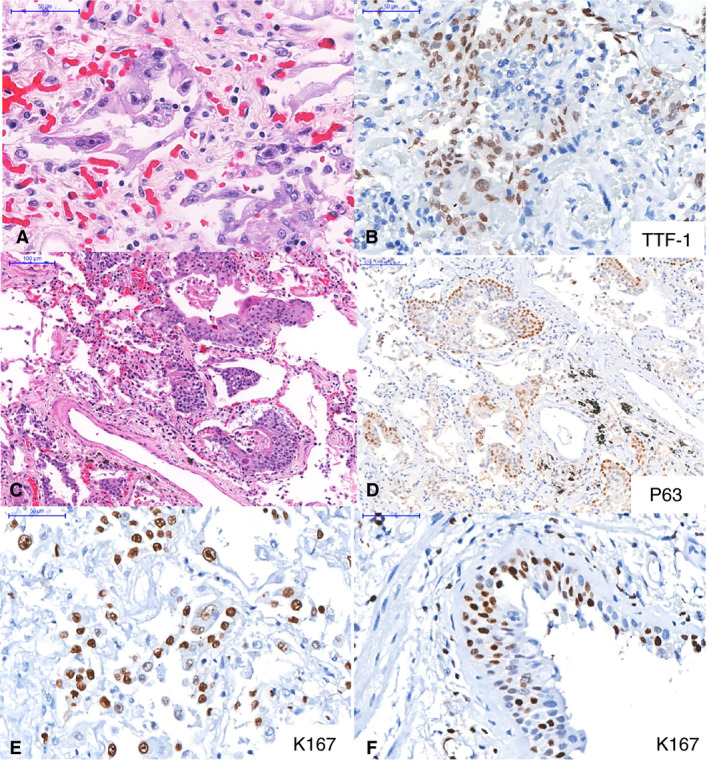
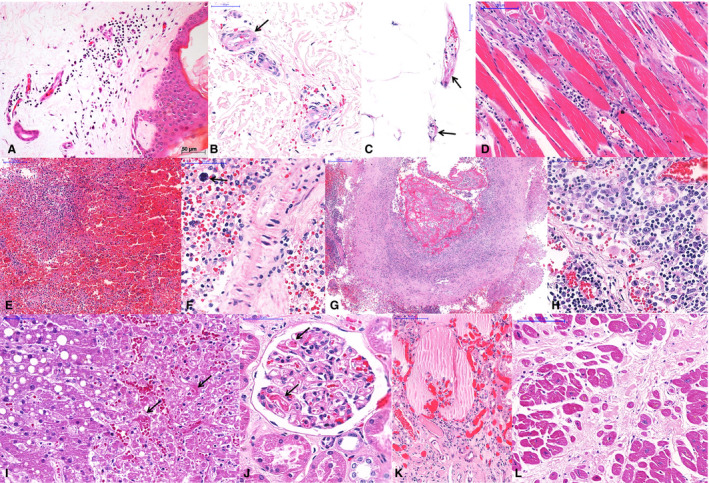
Methods and results: We used MIA-US for tissue sampling of the lungs, liver, heart, kidneys, spleen, brain, skin, skeletal muscle and testis for histology, and reverse transcription polymerase chain reaction to detect severe acute respiratory syndrome coronavirus 2 RNA. All patients showed exudative/proliferative diffuse alveolar damage. There were intense pleomorphic cytopathic effects on the respiratory epithelium, including airway and alveolar cells. Fibrinous thrombi in alveolar arterioles were present in eight patients, and all patients showed a high density of alveolar megakaryocytes. Small thrombi were less frequently observed in the glomeruli, spleen, heart, dermis, testis, and liver sinusoids. The main systemic findings were associated with comorbidities, age, and sepsis, in addition to possible tissue damage due to the viral infection, such as myositis, dermatitis, myocarditis, and orchitis.
Conclusions: MIA-US is safe and effective for the study of severe COVID-19. Our findings show that COVID-19 is a systemic disease causing major events in the lungs and with involvement of various organs and tissues. Pulmonary changes result from severe epithelial injury and microthrombotic vascular phenomena. These findings indicate that both epithelial and vascular injury should be addressed in therapeutic approaches.
Keywords: COVID-19; SARS-CoV-2; autopsy; diffuse alveolar damage; lung pathology; minimally invasive autopsy.
© 2020 John Wiley & Sons Ltd.
Conflict of interest statement
The authors have no conflicts of interest.
Figures
References
-
- World Health Organization . Coronavirus disease 2019 (COVID‐19) situation Report—101. Available at: https://www.who.int/docs/default‐source/coronaviruse/situation‐reports/2... (accessed 1 May 2020).
-
- Ministério da Saúde‐Secretaria de Vigilância em Saúde . Boletim Epidemiológico Especial—14|SE 18—26 de abril de 2020. Available at: https://portalarquivos.saude.gov.br/images/pdf/2020/April/27/2020‐04‐27‐... (accessed 29 April 2020).
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Miscellaneous
