

Sepsis Associated Delirium
- PMID: 32443606
- PMCID: PMC7279289
- DOI: 10.3390/medicina56050240
Sepsis Associated Delirium
Abstract
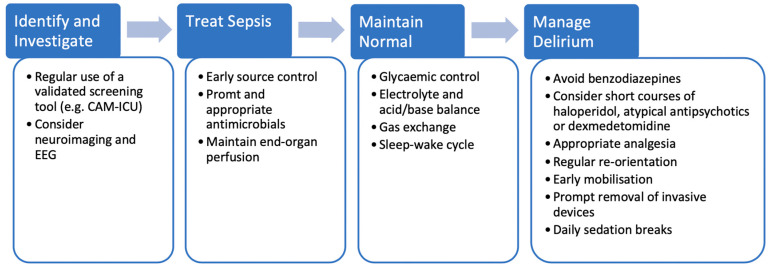
Sepsis is a potentially life-threatening condition caused by a systemic dysregulated host response to infection. The brain is particularly susceptible to the effects of sepsis with clinical manifestations ranging from mild confusion to a deep comatose state. Sepsis-associated delirium (SAD) is a cerebral manifestation commonly occurring in patients with sepsis and is thought to occur due to a combination of neuroinflammation and disturbances in cerebral perfusion, the blood brain barrier (BBB) and neurotransmission. The neurological impairment associated with SAD can persist for months or even longer, after the initial septic episode has subsided which may impair the rehabilitation potential of sepsis survivors. Early identification and treatment of the underlying sepsis is key in the management of SAD as once present it can be difficult to control. Through the regular use of validated screening tools for delirium, cases of SAD can be identified early; this allows potentially aggravating factors to be addressed promptly. The usefulness of biomarkers, neuroimaging and electroencephalopathy (EEG) in the diagnosis of SAD remains controversial. The Society of Critical Care Medicine (SCCM) guidelines advise against the use of medications to treat delirium unless distressing symptoms are present or it is hindering the patient's ability to wean from organ support.
Keywords: ICU; delirium; dexmedetomidine; sepsis.
Conflict of interest statement
The authors declare no conflicts of interest.
Figures
References
-
- Hughes C.G., Morandi A., Girard T.D., Riedel B., Thompson J.L., Shintani A.K., Pun B.T., Ely E.W., Pandharipande P.P. Association between endothelial dysfunction and acute brain dysfunction during critical illness. Anesthesiology. 2013;118:631–639. doi: 10.1097/ALN.0b013e31827bd193. - DOI - PMC - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
