

Quantifying the Genetic Basis of Marfan Syndrome Clinical Variability
- PMID: 32443863
- PMCID: PMC7288268
- DOI: 10.3390/genes11050574
Quantifying the Genetic Basis of Marfan Syndrome Clinical Variability
Abstract
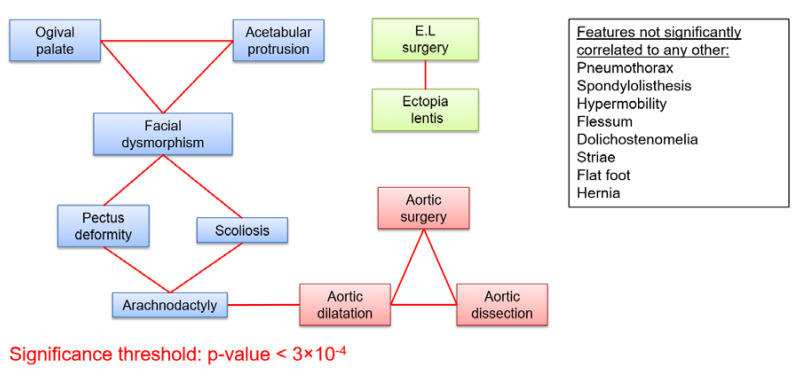
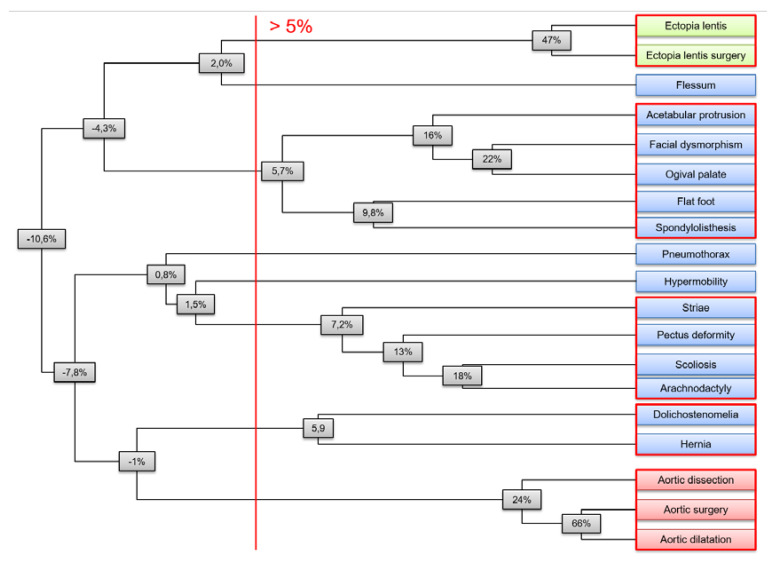
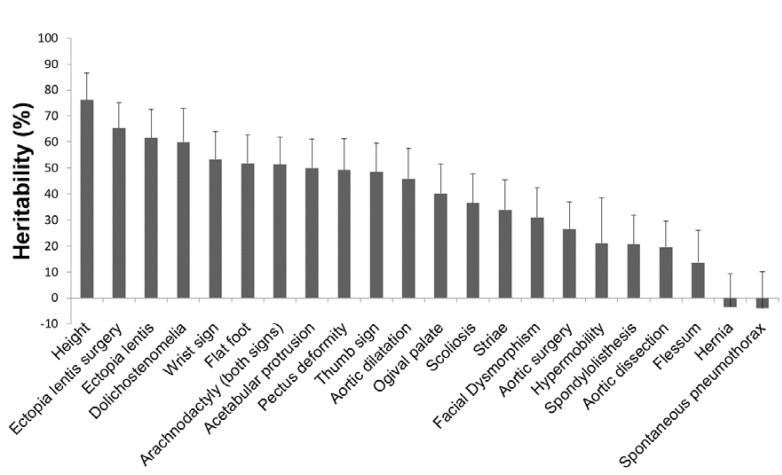
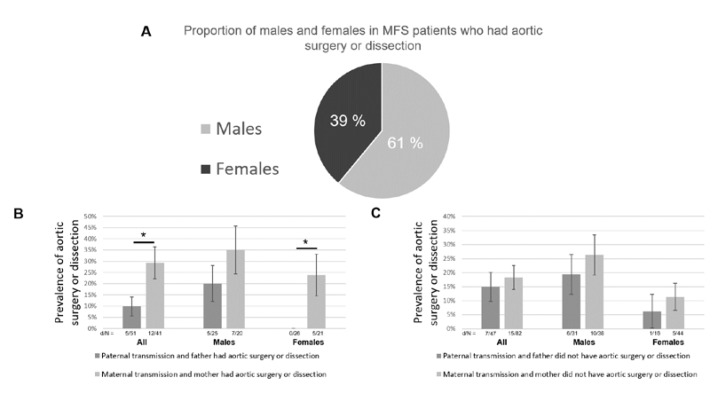
Marfan syndrome (MFS) is an autosomal dominant connective tissue disorder with considerable inter- and intra-familial clinical variability. The contribution of inherited modifiers to variability has not been quantified. We analyzed the distribution of 23 clinical features in 1306 well-phenotyped MFS patients carrying FBN1 mutations. We found strong correlations between features within the same system (i.e., ophthalmology vs. skeletal vs. cardiovascular) suggesting common underlying determinants, while features belonging to different systems were largely uncorrelated. We adapted a classical quantitative genetics model to estimate the heritability of each clinical feature from phenotypic correlations between relatives. Most clinical features showed strong familial aggregation and high heritability. We found a significant contribution by the major locus on the phenotypic variance only for ectopia lentis using a new strategy. Finally, we found evidence for the "Carter effect" in the MFS cardiovascular phenotype, which supports a polygenic model for MFS cardiovascular variability and indicates additional risk for children of MFS mothers with an aortic event. Our results demonstrate that an important part of the phenotypic variability in MFS is under the control of inherited modifiers, widely shared between features within the same system, but not among different systems. Further research must be performed to identify genetic modifiers of MFS severity.
Keywords: fibrillin; heritability; marfan; modifiers.
Conflict of interest statement
The authors declare no conflict of interest. The funders had no role in the design of the study; in the collection, analyses, or interpretation of data; in the writing of the manuscript, or in the decision to publish the results.
Figures
References
-
- Milleron O., Arnoult F., Delorme G., Detaint D., Pellenc Q., Raffoul R., Tchitchinadze M., Langeois M., Guien C., Beroud C., et al. Pathogenic FBN1 Genetic Variation and Aortic Dissection in Patients With Marfan Syndrome. J. Am. Coll. Cardiol. 2020;75:843–853. doi: 10.1016/j.jacc.2019.12.043. - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Medical
