

Genomic Methods Identify Homologous Recombination Deficiency in Pancreas Adenocarcinoma and Optimize Treatment Selection
- PMID: 32444418
- PMCID: PMC7380542
- DOI: 10.1158/1078-0432.CCR-20-0418
Genomic Methods Identify Homologous Recombination Deficiency in Pancreas Adenocarcinoma and Optimize Treatment Selection
Abstract
Purpose: Genomic methods can identify homologous recombination deficiency (HRD). Rigorous evaluation of their outcome association to DNA damage response-targeted therapies like platinum in pancreatic ductal adenocarcinoma (PDAC) is essential in maximizing therapeutic outcome.
Experimental design: We evaluated progression-free survival (PFS) and overall survival (OS) of patients with advanced-stage PDAC, who had both germline- and somatic-targeted gene sequencing. Homologous recombination gene mutations (HRm) were evaluated: BRCA1, BRCA2, PALB2, ATM, BAP1, BARD1, BLM, BRIP1, CHEK2, FAM175A, FANCA, FANCC, NBN, RAD50, RAD51, RAD51C, and RTEL1 HRm status was grouped as: (i) germline versus somatic; (ii) core (BRCAs and PALB2) versus non-core (other HRm); and (iii) monoallelic versus biallelic. Genomic instability was compared using large-scale state transition, signature 3, and tumor mutation burden.
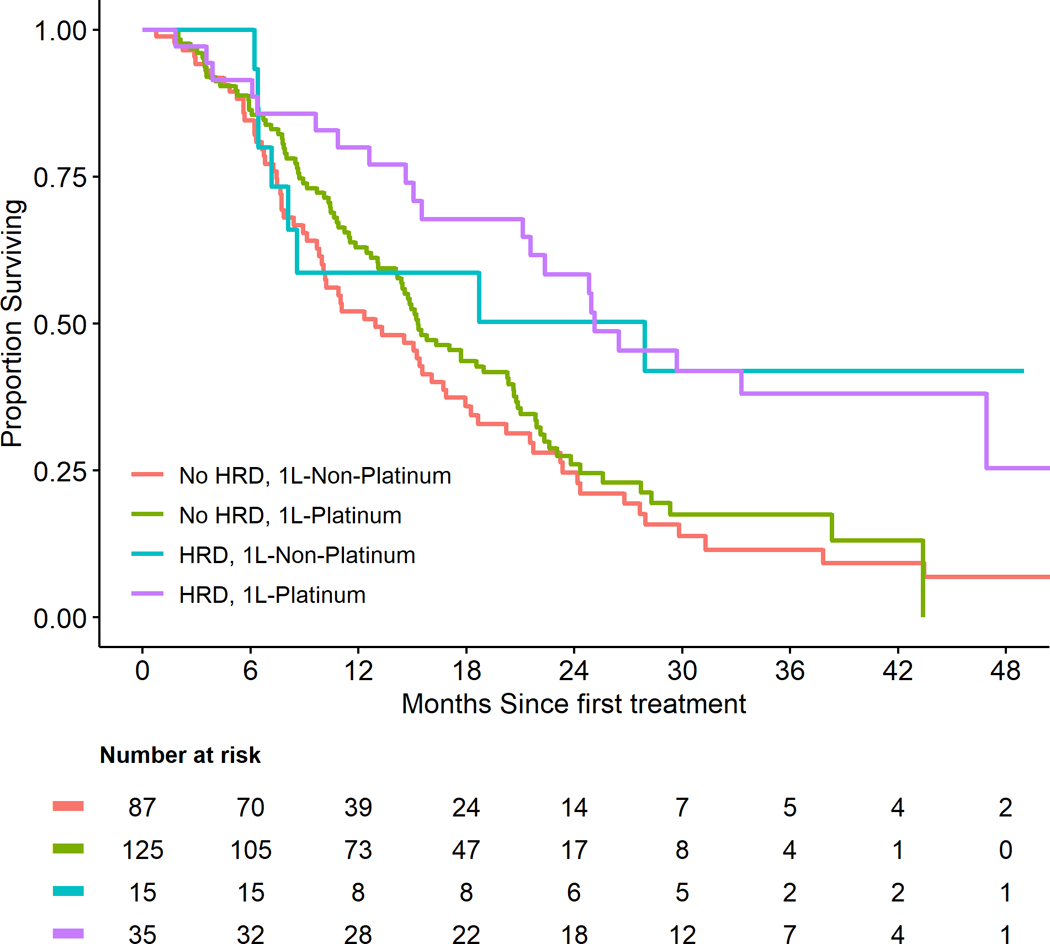
Results: Among 262 patients, 50 (19%) had HRD (15% germline and 4% somatic). Both groups were analyzed together due to lack of difference in their genomic instability and outcome. Median [95% confidence interval (CI)] follow-up was 21.9 (1.4-57.0) months. Median OS and PFS were 15.5 (14.6-19) and 7 (6.1-8.1) months, respectively. Patients with HRD had improved PFS compared with no HRD when treated with first-line (1L) platinum [HR, 0.44 (95% CI: 0.29-0.67); P < 0.01], but not with 1L-non-platinum. Multivariate analysis showed HRD patients had improved OS regardless of their first-line treatment, but most had platinum exposure during their course. Biallelic HRm (11%) and core HRm (12%) had higher genomic instability, which translated to improved PFS on first-line platinum (1L-platinum) versus 1L-non-platinum.
Conclusions: Pathogenic HRm identifies HRD in patients with PDAC with the best outcome when treated with 1L-platinum. Biallelic HRm and core HRm further enriched benefit from 1L-platinum from HRD.
©2020 American Association for Cancer Research.
Conflict of interest statement
Figures



References
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
Research Materials
Miscellaneous
